Вам также может понравиться
- Test Bank For 3 2 1 Code It 2020 8th Edition Michelle Green Full DownloadДокумент24 страницыTest Bank For 3 2 1 Code It 2020 8th Edition Michelle Green Full Downloadrobertabergmjnxqrasct100% (43)
- Application of Functional Orthodontic Appliances To Treatment of Mandibular Retrusion Syndrome PDFДокумент18 страницApplication of Functional Orthodontic Appliances To Treatment of Mandibular Retrusion Syndrome PDFThu Trang Pham100% (1)
- Culture and HealthДокумент3 страницыCulture and HealthEstiloОценок пока нет
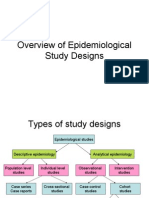
- Overview of Epidemiological Study DesignsДокумент16 страницOverview of Epidemiological Study DesignsLakshmi Seth100% (2)
- The Aspects of Gene TherapyДокумент15 страницThe Aspects of Gene TherapyLaleth Mendoza Ojales0% (1)
- Disusun: 1519 777 14 371: A.Asriwahyuni Lestari Fidya Novita Sari 15 19 777 14 361 PembimbingДокумент15 страницDisusun: 1519 777 14 371: A.Asriwahyuni Lestari Fidya Novita Sari 15 19 777 14 361 PembimbingfidyaОценок пока нет
- Fixed Drug EruptionsДокумент16 страницFixed Drug EruptionsfidyaОценок пока нет
- Sulphasalazine Induced Toxic Epidermal Necrolysis A Case ReportДокумент3 страницыSulphasalazine Induced Toxic Epidermal Necrolysis A Case ReportIOSR Journal of PharmacyОценок пока нет
- MP Asociado A SJSДокумент2 страницыMP Asociado A SJSMc PiryxОценок пока нет
- Nifedipine-Lnduced Erythema Multiforme: Sarah) - Barker, Charles Bayliff, Mccormack and DilworthДокумент3 страницыNifedipine-Lnduced Erythema Multiforme: Sarah) - Barker, Charles Bayliff, Mccormack and DilworthIrma NoviantiОценок пока нет
- Ijfp 2332 287X 03 503Документ4 страницыIjfp 2332 287X 03 503diijah678Оценок пока нет
- Daftar PustakaДокумент1 страницаDaftar PustakasherlyОценок пока нет
- Wells Syndrome (Eosinophilic Cellulitis) : Proposed Diagnostic Criteria and A Literature Review of The Drug-Induced VariantДокумент8 страницWells Syndrome (Eosinophilic Cellulitis) : Proposed Diagnostic Criteria and A Literature Review of The Drug-Induced VariantAnamaria IuoraşОценок пока нет
- Toxic Epidermal Necrolysis A Case ReportДокумент3 страницыToxic Epidermal Necrolysis A Case ReportResearch ParkОценок пока нет
- Tiwari 2013Документ8 страницTiwari 2013Stella SunurОценок пока нет
- Ten N Sjs ReviewДокумент5 страницTen N Sjs ReviewNantini GopalОценок пока нет
- Toxic Epidermal Necrolysis: BackgroundДокумент36 страницToxic Epidermal Necrolysis: BackgroundGita AmeliaОценок пока нет
- TEN and SJSДокумент8 страницTEN and SJSreyhanrrОценок пока нет
- Chronic Urticaria Clinical Presentation - History, Physical Examination, ComplicationsДокумент5 страницChronic Urticaria Clinical Presentation - History, Physical Examination, ComplicationsOgy SkillОценок пока нет
- 1421236494A Case of Neurodermitis Circumscripta With Generalized PruritisДокумент3 страницы1421236494A Case of Neurodermitis Circumscripta With Generalized PruritisAryantii AntyОценок пока нет
- Original Article Retrospective Analysis of Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis Over A Period of 10 YearsДокумент6 страницOriginal Article Retrospective Analysis of Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis Over A Period of 10 YearssyalalaaalalaaaОценок пока нет
- Revisión DRESS PDFДокумент20 страницRevisión DRESS PDFPaulaGallardoZegersОценок пока нет
- Stevens-Johnson SyndromeДокумент4 страницыStevens-Johnson SyndromeBelleОценок пока нет
- Dobson 2017Документ5 страницDobson 2017Stella SunurОценок пока нет
- Lichen Planus-Like Drug Eruptions Due To B-BlockersДокумент5 страницLichen Planus-Like Drug Eruptions Due To B-BlockersRudnapon AmornlaksananonОценок пока нет
- Adverse Cutaneous Drug Eruptions: Current Understanding: ReviewДокумент12 страницAdverse Cutaneous Drug Eruptions: Current Understanding: ReviewasdasdОценок пока нет
- Refarat EcthymaДокумент28 страницRefarat EcthymaFujiFebОценок пока нет
- Alergic DermatithisДокумент4 страницыAlergic DermatithisFrancois Donatien De SadeОценок пока нет
- 4556Документ2 страницы4556Yona LadyventiniОценок пока нет
- Review of Toxic Epidermal NecrolysisДокумент10 страницReview of Toxic Epidermal NecrolysisNurfitri ZuhruhurОценок пока нет
- Neurodermatitis (Lichen Simplex Chronic)Документ26 страницNeurodermatitis (Lichen Simplex Chronic)Yusran Ady FitrahОценок пока нет
- Variants of Erythema Multiforme: A Case Report and Literature ReviewДокумент8 страницVariants of Erythema Multiforme: A Case Report and Literature Reviewranz ibonkОценок пока нет
- The Dress Syndrome A Literature Review PDFДокумент7 страницThe Dress Syndrome A Literature Review PDFdajev1budaz2100% (1)
- Dupilumab Treatment in Adults With Moderate-to-Severe Atopic DermatitisДокумент10 страницDupilumab Treatment in Adults With Moderate-to-Severe Atopic DermatitisDwi Putri SimamoraОценок пока нет
- DR - Faiq Update Revised 2new BDДокумент34 страницыDR - Faiq Update Revised 2new BDamereОценок пока нет
- BJD 12501Документ10 страницBJD 12501abdulariifОценок пока нет
- 1996 Orf in A Rural Region of SpainДокумент4 страницы1996 Orf in A Rural Region of SpainlpozohОценок пока нет
- Adverse Cutaneous Drug EruptioДокумент13 страницAdverse Cutaneous Drug EruptioPeroquieОценок пока нет
- SJS (Jurnal)Документ6 страницSJS (Jurnal)FerryRoferdiОценок пока нет
- Sporadic Colonic Polyposis and Adenocarcinoma Associated With Lymphoblastic and Large B-Cell Lymphoma in A Young Male Patient: A Case Report.Документ3 страницыSporadic Colonic Polyposis and Adenocarcinoma Associated With Lymphoblastic and Large B-Cell Lymphoma in A Young Male Patient: A Case Report.pancholarpancholarОценок пока нет
- Regi Scar Score DressДокумент7 страницRegi Scar Score DressLinda PurwasihОценок пока нет
- Zaccaria 2006Документ2 страницыZaccaria 2006dermatom dervenОценок пока нет
- Toxic Epidermal Necrolysis: A Paradigm of Critical IllnessДокумент10 страницToxic Epidermal Necrolysis: A Paradigm of Critical IllnessViolett LiebeОценок пока нет
- Kulit Kulit KulitДокумент15 страницKulit Kulit KulitFarahnisa MappasissiОценок пока нет
- Dihematoporphyrin Ether-Induced Photosensitivity in Laryngeal Papilloma PatientsДокумент8 страницDihematoporphyrin Ether-Induced Photosensitivity in Laryngeal Papilloma PatientsDayse CSMОценок пока нет
- Allopurinol Induced Steven-Jonson Syndrome: Case ReportДокумент5 страницAllopurinol Induced Steven-Jonson Syndrome: Case ReportNoraPutriОценок пока нет
- Treatment of Chancroid With Enoxacin: ReferencesДокумент3 страницыTreatment of Chancroid With Enoxacin: References7dsp7xvs8dОценок пока нет
- 2018 Severe Cutaneous Adverse Drug Reactions - Presentation, Risk Factors, and ManagementДокумент9 страниц2018 Severe Cutaneous Adverse Drug Reactions - Presentation, Risk Factors, and ManagementpablopabloortizortizОценок пока нет
- Johnson 2004Документ9 страницJohnson 2004Abdul Wahab 2008126345Оценок пока нет
- Morbili: Residen Pembimbing Dr. Maryam Kusumawati Supervisor Dr. Safruddin Amin, SP - KK (K), MARS., FINSDVДокумент15 страницMorbili: Residen Pembimbing Dr. Maryam Kusumawati Supervisor Dr. Safruddin Amin, SP - KK (K), MARS., FINSDVnabillaОценок пока нет
- Psoriais PDF NemДокумент14 страницPsoriais PDF NemFabiola VillanuevaОценок пока нет
- Prurigo Nodularis of HydeДокумент12 страницPrurigo Nodularis of HydeAugusto MonjardimОценок пока нет
- Diabetes and Pruritus: Parastoo Babakinejad, Shernaz WaltonДокумент2 страницыDiabetes and Pruritus: Parastoo Babakinejad, Shernaz WaltonCelcius ButandyОценок пока нет
- Jurnal Tonsil Limfoma Non HodgkinДокумент5 страницJurnal Tonsil Limfoma Non HodgkinAhmad RamadhanuОценок пока нет
- Daftar Pustaka: Indonesia. Eritema Multiforme/sindrom Steven-Johnson/NekrolisisДокумент1 страницаDaftar Pustaka: Indonesia. Eritema Multiforme/sindrom Steven-Johnson/NekrolisisErfian PrissantikaОценок пока нет
- Drug Rash With Eosinophilia and Systemic Symptoms PDFДокумент3 страницыDrug Rash With Eosinophilia and Systemic Symptoms PDFclarissa1010Оценок пока нет
- Drug Rash With Eosinophilia and Systemic Symptoms PDFДокумент3 страницыDrug Rash With Eosinophilia and Systemic Symptoms PDFclarissa1010Оценок пока нет
- SweetsyndromeДокумент2 страницыSweetsyndromeDrSharan AnatomistОценок пока нет
- Atopic Dermatitis 2013Документ32 страницыAtopic Dermatitis 2013Bagus Maha ParadipaОценок пока нет
- Review On Terminalia ChebulaДокумент2 страницыReview On Terminalia ChebulaAman SrivastavaОценок пока нет
- Metoprolol Succinate Therapy Associated With Erythema MultiformeДокумент2 страницыMetoprolol Succinate Therapy Associated With Erythema MultiformeChikita Artia SariОценок пока нет
- Recurrent Erythema Multiforme: A Dental Case Report: ReviewДокумент4 страницыRecurrent Erythema Multiforme: A Dental Case Report: Reviewjenn_1228Оценок пока нет
- 329-Article Text-1006-2-10-20200429Документ5 страниц329-Article Text-1006-2-10-20200429Drina PaglinawanОценок пока нет
- 51 Uysal EtalДокумент4 страницы51 Uysal EtaleditorijmrhsОценок пока нет
- Data PetaДокумент4 страницыData PetaEkha SaraswatiОценок пока нет
- Eka Saraswati Tawainella-Starting School at An Early AgeДокумент1 страницаEka Saraswati Tawainella-Starting School at An Early AgeEkha SaraswatiОценок пока нет
- Eka Saraswati Tawainella - Maps IslandДокумент1 страницаEka Saraswati Tawainella - Maps IslandEkha SaraswatiОценок пока нет
- Eka Saraswati Tawainella-Starting School at An Early AgeДокумент1 страницаEka Saraswati Tawainella-Starting School at An Early AgeEkha SaraswatiОценок пока нет
- PBL AcaДокумент1 страницаPBL AcaEkha SaraswatiОценок пока нет
- Eka Saraswati - Salmon Life CycleДокумент1 страницаEka Saraswati - Salmon Life CycleEkha SaraswatiОценок пока нет
- Eka Saraswati Tawainella-Starting School at An Early AgeДокумент1 страницаEka Saraswati Tawainella-Starting School at An Early AgeEkha SaraswatiОценок пока нет
- Transport PercentageДокумент1 страницаTransport PercentageEkha SaraswatiОценок пока нет
- Types of Skin LesionsДокумент3 страницыTypes of Skin LesionsEkha SaraswatiОценок пока нет
- Seborrheic DermatitisДокумент6 страницSeborrheic DermatitisEkha SaraswatiОценок пока нет
- Malignant Phyllodes Tumor of The Breast: Treatment and PrognosisДокумент6 страницMalignant Phyllodes Tumor of The Breast: Treatment and PrognosisEkha SaraswatiОценок пока нет
- Langkah Diagnosis KulitДокумент4 страницыLangkah Diagnosis KulitEkha SaraswatiОценок пока нет
- Seborrheic DermatitisДокумент6 страницSeborrheic DermatitisEkha SaraswatiОценок пока нет
- FR Radius UlnaДокумент49 страницFR Radius UlnaEkha SaraswatiОценок пока нет
- Bhs - Inggris PutriДокумент1 страницаBhs - Inggris PutriEkha SaraswatiОценок пока нет
- Cover PageДокумент2 страницыCover PageEkha SaraswatiОценок пока нет
- Daftar Hadir Pembacaan Textbook Reading Koas Bagian Orthopedi Dan Traumatologi Fakultas Kedokteran Universitas HasanuddinДокумент2 страницыDaftar Hadir Pembacaan Textbook Reading Koas Bagian Orthopedi Dan Traumatologi Fakultas Kedokteran Universitas HasanuddinEkha SaraswatiОценок пока нет
- Bhs - Inggris PutriДокумент1 страницаBhs - Inggris PutriEkha SaraswatiОценок пока нет
- Fixed Drug Eruption: Pathogenesis and Diagnostic Tests.: Author InformationДокумент2 страницыFixed Drug Eruption: Pathogenesis and Diagnostic Tests.: Author InformationEkha SaraswatiОценок пока нет
- Concept Map Paper Steve NaraineДокумент6 страницConcept Map Paper Steve Naraineapi-283596053Оценок пока нет
- A Simplified Method For Fabricating Customized Arch Form: Clinical InnovationДокумент3 страницыA Simplified Method For Fabricating Customized Arch Form: Clinical InnovationPrimandita NugrahaОценок пока нет
- Health Care Delivery System 1Документ21 страницаHealth Care Delivery System 1Carson BirthОценок пока нет
- Testicular PainДокумент16 страницTesticular PainkdwazirОценок пока нет
- Distaclor Granules For Suspension 125mg/5ml & 250mg/5mlДокумент2 страницыDistaclor Granules For Suspension 125mg/5ml & 250mg/5mlfirdausazinun8684Оценок пока нет
- RotundaAmbulatoryHysteroscopyService at ConnollyHospitalДокумент34 страницыRotundaAmbulatoryHysteroscopyService at ConnollyHospitalAndreeaОценок пока нет
- MDHA Write-Up For Prospective StudentsДокумент1 страницаMDHA Write-Up For Prospective StudentsprashantОценок пока нет
- Group Mediclaim Policy Coverages For Employees of Century PlyДокумент2 страницыGroup Mediclaim Policy Coverages For Employees of Century PlyUDAYОценок пока нет
- The Story of Florence NightingaleДокумент2 страницыThe Story of Florence NightingaleBella RettobОценок пока нет
- EpidemiologyДокумент52 страницыEpidemiologyasdfsОценок пока нет
- World Health DayДокумент18 страницWorld Health DayRamandeep KaurОценок пока нет
- Nursing Process: Mrs. Sumaira Noreen Senior Nursing InstructorДокумент40 страницNursing Process: Mrs. Sumaira Noreen Senior Nursing InstructorSumaira NoreenОценок пока нет
- Week 3 Session 1 - Knife CrimeДокумент26 страницWeek 3 Session 1 - Knife CrimeAlejandro CardonaОценок пока нет
- ABCDE Assessment Exam: Eunice QuijanoДокумент3 страницыABCDE Assessment Exam: Eunice QuijanoQuijano GpokskieОценок пока нет
- A Carbohydrate-Restrictive Strategy Is Safer and As Efficient As Intensive Insulin Therapy in Critically Ill PatientsДокумент6 страницA Carbohydrate-Restrictive Strategy Is Safer and As Efficient As Intensive Insulin Therapy in Critically Ill PatientsTeresaОценок пока нет
- A Clinical Report On Partial Pulpotomy and Capping With Calcium Hydroxide in Permanent Incisors With Complicated Crown FractureДокумент6 страницA Clinical Report On Partial Pulpotomy and Capping With Calcium Hydroxide in Permanent Incisors With Complicated Crown Fractureroy sepОценок пока нет
- My New ThesisДокумент7 страницMy New ThesisAlla Yeswanth Dilip KumarОценок пока нет
- Hunting For Disease XДокумент9 страницHunting For Disease XPeter GoodsallОценок пока нет
- Research Essay 4Документ15 страницResearch Essay 4api-584378330Оценок пока нет
- Haramaya University College of Health and Medical ScienceДокумент39 страницHaramaya University College of Health and Medical Scienceani gadaОценок пока нет
- Service Learning Reflection PaperДокумент3 страницыService Learning Reflection Paperapi-297614673Оценок пока нет
- E/M Audit Form: Chart #Документ2 страницыE/M Audit Form: Chart #Anthony El HageОценок пока нет
- Chapter 23 HomeworkДокумент10 страницChapter 23 HomeworkKvn4N6Оценок пока нет
- Cancer4less Research Paper Ishmita VaishДокумент2 страницыCancer4less Research Paper Ishmita Vaishvaishjia23Оценок пока нет
- Ot Mental Health NutritionДокумент11 страницOt Mental Health Nutritionapi-340399319Оценок пока нет