Вам также может понравиться
- Treatment Modalities For Mood DisordersДокумент55 страницTreatment Modalities For Mood DisordersGlory MimiОценок пока нет
- Antidepressants MaterialДокумент5 страницAntidepressants MaterialxyzОценок пока нет
- AntidepressantsДокумент59 страницAntidepressantsanon_189054600100% (2)
- PsychopharmacologyДокумент32 страницыPsychopharmacologyCms CSU100% (1)
- 4.2 Psychotropic Drugs Used in PsychiatryДокумент32 страницы4.2 Psychotropic Drugs Used in PsychiatryAmar Nur Arif ZazuliОценок пока нет
- Types of DepressionДокумент12 страницTypes of DepressionKADAMBARIОценок пока нет
- Current Clinical Strategies: Handbook of Psychiatric DrugsДокумент72 страницыCurrent Clinical Strategies: Handbook of Psychiatric Drugsmike116Оценок пока нет
- PA 644 - M2 LecturesДокумент412 страницPA 644 - M2 LectureskatОценок пока нет
- Psycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsДокумент29 страницPsycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsPoonam RanaОценок пока нет
- Antidepressant DrugsДокумент21 страницаAntidepressant DrugsKashis SharmaОценок пока нет
- Anti Depressants FinalДокумент61 страницаAnti Depressants FinalAuthor Nauman Shad100% (1)
- Drug Abuse and Drug Dependence: DR Keli F Med III LecturesДокумент49 страницDrug Abuse and Drug Dependence: DR Keli F Med III LecturestheintrovОценок пока нет
- Nicotine Related DisordersДокумент74 страницыNicotine Related DisordersKuldeep singhОценок пока нет
- Moca Vs MMSEДокумент2 страницыMoca Vs MMSEYw LiuОценок пока нет
- Psychopharmacology NewestДокумент43 страницыPsychopharmacology NewestRegina PunОценок пока нет
- Antidepressants and AntipsychoticsДокумент50 страницAntidepressants and AntipsychoticsPintu Bhushan MitraОценок пока нет
- Substance Use DisordersДокумент28 страницSubstance Use DisordersAbdul NazarОценок пока нет
- Neuroleptics & AnxiolyticsДокумент65 страницNeuroleptics & AnxiolyticsAntonPurpurovОценок пока нет
- Etiopathogenesis of DeliriumДокумент36 страницEtiopathogenesis of DeliriumAarti Gupta100% (1)
- DELIRIUM PresentationДокумент26 страницDELIRIUM PresentationAnkush Sharma100% (1)
- CEP BPSD Discussion Guide ENG RFCG Updated2019 PDFДокумент8 страницCEP BPSD Discussion Guide ENG RFCG Updated2019 PDFM.DalaniОценок пока нет
- "Neurotransmitter": Supporting Lecturer: NOVIA SINATA, M.Si, AptДокумент24 страницы"Neurotransmitter": Supporting Lecturer: NOVIA SINATA, M.Si, AptAmoxicilliartha RivanolaОценок пока нет
- Geriatric Giants - DR SeymourДокумент108 страницGeriatric Giants - DR SeymourSharon Mallia100% (1)
- Medical Mimics 2016Документ24 страницыMedical Mimics 2016Susan Redmond-VaughtОценок пока нет
- Delirium: EpidemiologyДокумент8 страницDelirium: EpidemiologyNunuОценок пока нет
- INTRODUCTION TO NEUROPHARMACOLOGYyyДокумент27 страницINTRODUCTION TO NEUROPHARMACOLOGYyyEbad RazviОценок пока нет
- Cognitive Disorders PresentationДокумент70 страницCognitive Disorders PresentationWasiu AfoloabiОценок пока нет
- Sudden Onset (Within 2 Weeks) of at Least One of TheДокумент2 страницыSudden Onset (Within 2 Weeks) of at Least One of TheNeicole BandalaОценок пока нет
- Summary of Product Characteristics: PosologyДокумент9 страницSummary of Product Characteristics: Posologyddandan_2Оценок пока нет
- Tranylcypromine in Mind Part II - Review of Clinical PH - 2017 - European Neuro PDFДокумент18 страницTranylcypromine in Mind Part II - Review of Clinical PH - 2017 - European Neuro PDFdanilomarandolaОценок пока нет
- Pharmacology Workbook Class of 20 20: (Revised: March, 2018)Документ22 страницыPharmacology Workbook Class of 20 20: (Revised: March, 2018)Navdeep RandhawaОценок пока нет
- Assessment and Management of Agitation in Psychiatry Expert ConsensusДокумент44 страницыAssessment and Management of Agitation in Psychiatry Expert ConsensusPablo RamirezОценок пока нет
- Receptors Ionchannel TransporterДокумент58 страницReceptors Ionchannel TransporterDeepu Vijay100% (1)
- NeurotransmittersДокумент29 страницNeurotransmittersashupathakaОценок пока нет
- Neurobiology and BehaviorДокумент24 страницыNeurobiology and BehaviorNaveen Eldose100% (1)
- TramadolДокумент3 страницыTramadolKaren Viviene Aberilla CincoОценок пока нет
- AnxietyДокумент5 страницAnxietyJohn HolmesОценок пока нет
- Chapter 7 Study GuideДокумент4 страницыChapter 7 Study GuidejbradeeОценок пока нет
- Mental Health - PsychopharmacologyДокумент4 страницыMental Health - PsychopharmacologyRenetria DrakeОценок пока нет
- Anti PsychoticsДокумент34 страницыAnti Psychotics88AKKОценок пока нет
- Investigations in PsychiatryДокумент59 страницInvestigations in Psychiatrykiran mahal100% (1)
- Anidepressant Drugs: Pratik KhanalДокумент37 страницAnidepressant Drugs: Pratik KhanalPratik Khanal100% (1)
- Antidepressant AgentsДокумент38 страницAntidepressant AgentsdidiОценок пока нет
- Tranylcypromine in Mind Part I - Review of P - 2017 - European Neuropsychopharm PDFДокумент17 страницTranylcypromine in Mind Part I - Review of P - 2017 - European Neuropsychopharm PDFdanilomarandolaОценок пока нет
- Sample Pages of Pharmacology 4th EditionДокумент25 страницSample Pages of Pharmacology 4th EditionskОценок пока нет
- Neurotransmitters in Schizophrenia: Dr. Adel El SheshaiДокумент47 страницNeurotransmitters in Schizophrenia: Dr. Adel El SheshaielvinegunawanОценок пока нет
- Anti-Depressants: Soumya Mary 1 Year MSC (N)Документ22 страницыAnti-Depressants: Soumya Mary 1 Year MSC (N)Salman HabeebОценок пока нет
- Inhibitors of MAO-A and MAO-B in Psychiatry and NeurologyДокумент27 страницInhibitors of MAO-A and MAO-B in Psychiatry and NeurologySergeyОценок пока нет
- Glutamate & Gaba: NeurotransmittersДокумент33 страницыGlutamate & Gaba: NeurotransmittersPanchitaJuarezОценок пока нет
- Drugs For NeurolepticsДокумент1 страницаDrugs For Neurolepticssyamil_daudОценок пока нет
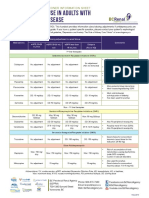
- Antidepressant Use in Adults With Chronic Kidney DiseaseДокумент1 страницаAntidepressant Use in Adults With Chronic Kidney DiseaseAzhar Ali100% (1)
- 1 - Signs and Symptoms of Mental Illness-PartДокумент49 страниц1 - Signs and Symptoms of Mental Illness-PartAljoker FarragОценок пока нет
- Antipsychotic or Neuroleptic DrugsДокумент12 страницAntipsychotic or Neuroleptic Drugscamile buhanginОценок пока нет
- Schizophrenia: By: Zoya MoraniДокумент31 страницаSchizophrenia: By: Zoya Moranimed studentОценок пока нет
- PsychopharmacologyДокумент53 страницыPsychopharmacologypujarze4100% (1)
- Pristiq (Desvenlafaxine) Product Monograph For CanadaДокумент48 страницPristiq (Desvenlafaxine) Product Monograph For CanadajennabushОценок пока нет
- Schizophrenia OverviewДокумент8 страницSchizophrenia OverviewRiscky LauwОценок пока нет
- Drug Presentation: Manisha M.Sc. Nursing 1 Year Con IlbsДокумент57 страницDrug Presentation: Manisha M.Sc. Nursing 1 Year Con IlbsManisha ShakyaОценок пока нет
- Treatment Resistant OCD .Документ55 страницTreatment Resistant OCD .Dr viren SolankiОценок пока нет
- Internal Medicine - DermatologyДокумент125 страницInternal Medicine - DermatologySoleil DaddouОценок пока нет
- Fluids and ElectrolytesДокумент78 страницFluids and ElectrolytesSoleil DaddouОценок пока нет
- LMCC II GuideДокумент79 страницLMCC II GuideSoleil DaddouОценок пока нет
- Clinical Immunology and AllergyДокумент156 страницClinical Immunology and AllergySoleil DaddouОценок пока нет
- Dr. Noto ID HandoutДокумент35 страницDr. Noto ID HandoutSoleil DaddouОценок пока нет
- Dr. Noto ID HandoutДокумент35 страницDr. Noto ID HandoutSoleil DaddouОценок пока нет
- Complementary and Alternative Systems in PsychiatryДокумент131 страницаComplementary and Alternative Systems in Psychiatryganeshprabhuvk100% (1)
- Week4 PTC Formulary DispensingДокумент7 страницWeek4 PTC Formulary DispensingChunnie JakosalemОценок пока нет
- Metronidazole E.M.CДокумент1 страницаMetronidazole E.M.CCen Janber CabrillosОценок пока нет
- Verbeeck Lidose FormulationДокумент7 страницVerbeeck Lidose FormulationIntern 1Оценок пока нет
- Effect of Pharmacy Intervention To Patient With Polypharmacy - JournalДокумент7 страницEffect of Pharmacy Intervention To Patient With Polypharmacy - Journalanon_529380518Оценок пока нет
- Cardiopulmonary Resuscitation For Adults Pedia and InfantsДокумент35 страницCardiopulmonary Resuscitation For Adults Pedia and InfantsAnna Carmela Pillora MelendezОценок пока нет
- Aarnext List Portugese Product 22.09.2021Документ8 страницAarnext List Portugese Product 22.09.2021Fábio CorreiaОценок пока нет
- Jurnal ReadingДокумент13 страницJurnal Readingeliamegasari01Оценок пока нет
- Glyceryl Trinitrate (GTN) Infusion Chart For Chest Pain: (Or Affix Hospital Label Here)Документ2 страницыGlyceryl Trinitrate (GTN) Infusion Chart For Chest Pain: (Or Affix Hospital Label Here)wasim100% (1)
- Status Obat Dan Alkes Master 2019Документ166 страницStatus Obat Dan Alkes Master 2019AkramОценок пока нет
- Function of Each GearsДокумент6 страницFunction of Each GearsRacco Roy0% (1)
- Anaesthesia MCQ 2021Документ18 страницAnaesthesia MCQ 2021invisiblealchemist2007Оценок пока нет
- Pre Reg Pharmacists Last MinuteДокумент9 страницPre Reg Pharmacists Last MinuteBob BobОценок пока нет
- Drug Approval Manuscript India PDFДокумент10 страницDrug Approval Manuscript India PDFardhanputraОценок пока нет
- Efficacy of Pulsed Electromagnetic Therapy For Chronic Lower Back Pain: A Randomized, Double-Blind, Placebo-Controlled StudyДокумент8 страницEfficacy of Pulsed Electromagnetic Therapy For Chronic Lower Back Pain: A Randomized, Double-Blind, Placebo-Controlled StudyKyteОценок пока нет
- Djunizar Djamaludin, Rika Yulenda Sari: Januari 2021Документ10 страницDjunizar Djamaludin, Rika Yulenda Sari: Januari 2021Ag Istri Dwi ArdiiОценок пока нет
- MCQ Questions Lahore MedicalДокумент36 страницMCQ Questions Lahore MedicalClinicalTraining0% (1)
- Print TagsДокумент30 страницPrint TagspsychgypsyОценок пока нет
- Art Terapijske MetodeДокумент2 страницыArt Terapijske MetodeAleksandarRadojevićОценок пока нет
- Comparison of Hyperbaric Levobupivacaine/ Bupivacaine For Ceserean SectionДокумент6 страницComparison of Hyperbaric Levobupivacaine/ Bupivacaine For Ceserean SectionIJAR JOURNALОценок пока нет
- Antituberculous Therapy in Special SituationsДокумент8 страницAntituberculous Therapy in Special SituationsMobeen Raza100% (1)
- Mucosta Drug Interactions - MIMS MalaysiaДокумент4 страницыMucosta Drug Interactions - MIMS MalaysiaEsy LОценок пока нет
- Test Bank For Drug Use and Abuse 8th EditionДокумент36 страницTest Bank For Drug Use and Abuse 8th Editionoverspanchitter4abo100% (40)
- The 4 Different Types of TelepharmacyДокумент8 страницThe 4 Different Types of TelepharmacyAnonymous EAPbx6Оценок пока нет
- Prodrug (D.ashowq)Документ4 страницыProdrug (D.ashowq)علي الطياريОценок пока нет
- Massage in Ancient TimesДокумент4 страницыMassage in Ancient Timesgabby tolentinoОценок пока нет
- Wound Infection: Dr. Nisreen Anfanan DR .T.ZamzamiДокумент24 страницыWound Infection: Dr. Nisreen Anfanan DR .T.ZamzamimustaafОценок пока нет
- Laporan Penggunaan Maret 2020Документ6 страницLaporan Penggunaan Maret 2020siska thresiaОценок пока нет
- MedicationsДокумент13 страницMedicationsReynaKatОценок пока нет
- Review of Pharmacology (PGMEE) Paperback - 2018 (PDFDrive)Документ660 страницReview of Pharmacology (PGMEE) Paperback - 2018 (PDFDrive)xwendnla russiaОценок пока нет