Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Digest of Magtajas v. Pryce Properties Corp. (G.R. No. 111097)Документ2 страницыDigest of Magtajas v. Pryce Properties Corp. (G.R. No. 111097)Rafael Pangilinan94% (16)
- Joy James - Resisting State Violence - Radicalism, Gender, and Race in U.S. Culture-University of Minnesota Press (1996) PDFДокумент279 страницJoy James - Resisting State Violence - Radicalism, Gender, and Race in U.S. Culture-University of Minnesota Press (1996) PDFDiogo Marcal Cirqueira100% (1)
- Affidavit - ERRONEOUS ENTRY - BeronganДокумент1 страницаAffidavit - ERRONEOUS ENTRY - BeronganDiaz Law OfficeОценок пока нет
- 2012 Acute Bacterial Sinusitis in Children PDFДокумент7 страниц2012 Acute Bacterial Sinusitis in Children PDFAnnisa RahmaniОценок пока нет
- Application Form (JENESYS2.0)Документ3 страницыApplication Form (JENESYS2.0)Annisa RahmaniОценок пока нет
- Sleep Duration and Risk of Fatal and Nonfatal StrokeДокумент10 страницSleep Duration and Risk of Fatal and Nonfatal StrokeAnnisa RahmaniОценок пока нет
- Effect of Intravenous Nimodipine On Blood Pressure AndOutcome After Acute StrokeДокумент7 страницEffect of Intravenous Nimodipine On Blood Pressure AndOutcome After Acute StrokeAnnisa RahmaniОценок пока нет
- MS For StrokeДокумент9 страницMS For StrokeBagus Ngurah MahasenaОценок пока нет
- Jadwal Jaga Stase Abedah Rsud TanjungДокумент1 страницаJadwal Jaga Stase Abedah Rsud TanjungAnnisa RahmaniОценок пока нет
- Shafer FM PDFДокумент13 страницShafer FM PDFAnnisa RahmaniОценок пока нет
- Comparative Study of Outcomes of MicroscopicДокумент4 страницыComparative Study of Outcomes of MicroscopicAnnisa RahmaniОценок пока нет
- Treatment of Acute Otitis Media in ChildrenДокумент11 страницTreatment of Acute Otitis Media in ChildrenRamza Shiddiq As'AryОценок пока нет
- A Prospective Study Comparing The Results ofДокумент6 страницA Prospective Study Comparing The Results ofAnnisa RahmaniОценок пока нет
- Bilateral Same-Day Endoscopic Transcanal Cartilage Tympanoplasty Initial ResultsДокумент5 страницBilateral Same-Day Endoscopic Transcanal Cartilage Tympanoplasty Initial ResultsAnnisa RahmaniОценок пока нет
- 3 Jurnal Preterm LabourДокумент12 страниц3 Jurnal Preterm LabourAnnisa RahmaniОценок пока нет
- A Placebo-Controlled Trial of AntimicrobialДокумент11 страницA Placebo-Controlled Trial of AntimicrobialRamza Shiddiq As'AryОценок пока нет
- 49071Документ29 страниц49071Annisa RahmaniОценок пока нет
- 4 Jurnal Preterm LabourДокумент6 страниц4 Jurnal Preterm LabourAnnisa RahmaniОценок пока нет
- Homicide in Southern India-A Five-Year Retrospective StudyДокумент7 страницHomicide in Southern India-A Five-Year Retrospective StudyAnnisa RahmaniОценок пока нет
- Br. J. Anaesth. 2015 Reilly 482 3Документ2 страницыBr. J. Anaesth. 2015 Reilly 482 3Annisa RahmaniОценок пока нет
- Wolfe PTLДокумент42 страницыWolfe PTLriena456Оценок пока нет
- Premature LabourREДокумент27 страницPremature LabourREmahmnasОценок пока нет
- Prevent Predict Preterm Birth 2004Документ57 страницPrevent Predict Preterm Birth 2004Annisa RahmaniОценок пока нет
- 2R Jurnal ObgynДокумент5 страниц2R Jurnal ObgynAnnisa RahmaniОценок пока нет
- Preterm Labor and Birth ACOGДокумент3 страницыPreterm Labor and Birth ACOGPretty NoviannisaОценок пока нет
- Pi Premature LabourДокумент5 страницPi Premature LabourAnnisa RahmaniОценок пока нет
- Pattern of Injuries Among Two or Four Wheeler Occupants in Fatal Road Traffic InjuriesДокумент7 страницPattern of Injuries Among Two or Four Wheeler Occupants in Fatal Road Traffic InjuriesAnnisa RahmaniОценок пока нет
- 1 Jurnal Preterm LabourДокумент9 страниц1 Jurnal Preterm LabourAnnisa RahmaniОценок пока нет
- 5 Jurnal Preterm LabourДокумент8 страниц5 Jurnal Preterm LabourAnnisa RahmaniОценок пока нет
- Tocolysis For Women in Preterm Labour GuidlineДокумент13 страницTocolysis For Women in Preterm Labour GuidlineAbraham Dian Winarto100% (1)
- Agkegawat Daruratan BedahДокумент112 страницAgkegawat Daruratan BedahMirah WulandariОценок пока нет
- Preterm Labor Identification and TreatmentДокумент8 страницPreterm Labor Identification and TreatmentAnnisa RahmaniОценок пока нет
- 23 Phil LJ801Документ29 страниц23 Phil LJ801Agent BlueОценок пока нет
- Leonardi v. Chase National Bank DIGESTДокумент2 страницыLeonardi v. Chase National Bank DIGESTkathrynmaydevezaОценок пока нет
- Page 14 Why Did Cyrus Let Them GoДокумент5 страницPage 14 Why Did Cyrus Let Them Golawrece_acc5589Оценок пока нет
- On The Bondage of The WillДокумент576 страницOn The Bondage of The WillFrank LukeheartОценок пока нет
- Lic of India Nfifwi: Abhishek Kumar Anirbhan Hazra Anjana K C Rupali Nayak Shirshendu SahooДокумент26 страницLic of India Nfifwi: Abhishek Kumar Anirbhan Hazra Anjana K C Rupali Nayak Shirshendu SahooAnjana KcОценок пока нет
- Dillena vs. CAДокумент9 страницDillena vs. CALeizl A. VillapandoОценок пока нет
- Untitled DocumentДокумент40 страницUntitled DocumentVee Jay DeeОценок пока нет
- Format 9A: Applicable For Individual Loans Switchover From Existing Negative Spreadover RPLR To Higher Negative SpreadДокумент1 страницаFormat 9A: Applicable For Individual Loans Switchover From Existing Negative Spreadover RPLR To Higher Negative SpreadANANDARAJОценок пока нет
- AtheismДокумент2 страницыAtheismJonatan FrosthОценок пока нет
- Coming Out Monologues 2011 ScriptДокумент70 страницComing Out Monologues 2011 ScriptGuia PeraltaОценок пока нет
- G.R. No. 203766Документ125 страницG.R. No. 203766JacinthDelosSantosDelaCernaОценок пока нет
- Bsme Swimming Handbook 2018Документ6 страницBsme Swimming Handbook 2018api-318213408Оценок пока нет
- The Virtues of Syeda FatimaДокумент71 страницаThe Virtues of Syeda FatimaMubahilaTV Books & Videos OnlineОценок пока нет
- The State of Gujarat and Another Vs Shri Ambica Mills LTDДокумент12 страницThe State of Gujarat and Another Vs Shri Ambica Mills LTDUmmer Mohi ud dinОценок пока нет
- Negligence Cases (Torts - Dy)Документ11 страницNegligence Cases (Torts - Dy)Cathy Alcantara100% (1)
- MKII Hordes Forces Trollbloods PDFДокумент115 страницMKII Hordes Forces Trollbloods PDFleotardnimoyОценок пока нет
- "Phil Russo Is A Scam Artist," Says WardenДокумент3 страницы"Phil Russo Is A Scam Artist," Says WardenRoy WardenОценок пока нет
- The Cross in Johns Gospel PDFДокумент12 страницThe Cross in Johns Gospel PDFJoe ChavezОценок пока нет
- Praise and Worship Oct 10 2020Документ22 страницыPraise and Worship Oct 10 2020CrisDBОценок пока нет
- Past Perfect Simple and Past Perfect Continuous - AДокумент2 страницыPast Perfect Simple and Past Perfect Continuous - AFatima VenturaОценок пока нет
- Republic v. Rural Bank of Kabacan, Inc.Документ2 страницыRepublic v. Rural Bank of Kabacan, Inc.Yuri NishimiyaОценок пока нет
- The Infringement of Eritrean Sovereign Legal Right by The Anti-Eritrean Unity Speakers (Part 1)Документ38 страницThe Infringement of Eritrean Sovereign Legal Right by The Anti-Eritrean Unity Speakers (Part 1)Anonymous fdtcPX73g100% (1)
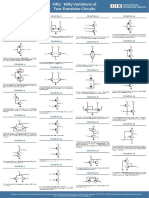
- Variations of Two-Transistor CircuitsДокумент2 страницыVariations of Two-Transistor CircuitsKoushik TeslaОценок пока нет
- Final Film ReflectionДокумент10 страницFinal Film ReflectionmorganflittОценок пока нет
- Minusma Daily Flights Schedule / Air Tasking Order Thursday, 20 April 2023 Aviation SectionДокумент15 страницMinusma Daily Flights Schedule / Air Tasking Order Thursday, 20 April 2023 Aviation SectionДенис ЮхненкоОценок пока нет
- Zernik V Connor Et Al (2:08-cv-01550) at The US District Court, Central District of California - DKT #031 Zernik's Request For Judicial Notice of Judge Bohm's Memorandum Opinion EtcДокумент85 страницZernik V Connor Et Al (2:08-cv-01550) at The US District Court, Central District of California - DKT #031 Zernik's Request For Judicial Notice of Judge Bohm's Memorandum Opinion EtcHuman Rights Alert - NGO (RA)Оценок пока нет
- Julian Masters - Training To PleasureДокумент167 страницJulian Masters - Training To PleasureBill Staropoli71% (7)