Вам также может понравиться
- Sciatic Nerve - IipptДокумент21 страницаSciatic Nerve - IipptPraneetha NouduriОценок пока нет
- An Update On Peroneal Nerve Entrapment and NeuropathyДокумент9 страницAn Update On Peroneal Nerve Entrapment and NeuropathyClara ViMiОценок пока нет
- Spinal Cord Deseases: Na ShaoДокумент38 страницSpinal Cord Deseases: Na ShaoArvindhanОценок пока нет
- Avascular Necrosis of The HipДокумент22 страницыAvascular Necrosis of The Hipbjpalmer100% (2)
- Choosehealth BrochureДокумент18 страницChoosehealth Brochureapi-487757844Оценок пока нет
- Co-Ordination: Prepared by Ahmed Shawky AliДокумент59 страницCo-Ordination: Prepared by Ahmed Shawky Alivenkata ramakrishnaiahОценок пока нет
- Coordination AssessmentДокумент30 страницCoordination AssessmentBhawna PalОценок пока нет
- Human Anatomy & PhysiologyДокумент72 страницыHuman Anatomy & PhysiologyJoie UrsalОценок пока нет
- Leg UlcerДокумент28 страницLeg UlcerRanindya PutriОценок пока нет
- Wrist FracturesДокумент3 страницыWrist FracturesFarah AzizahОценок пока нет
- Cervical SpondylosisДокумент9 страницCervical SpondylosisNurHidayah Borhanudin100% (1)
- Anxiety and Anxiety Disorders1Документ41 страницаAnxiety and Anxiety Disorders1Anne de VeraОценок пока нет
- Lecture 19 - Vessels and CirculationДокумент67 страницLecture 19 - Vessels and CirculationSasikala MohanОценок пока нет
- Claw HandДокумент23 страницыClaw HandAditya Pratama Saanin100% (1)
- Articular Neurophysiology: Presented by - Yogesh VyasДокумент15 страницArticular Neurophysiology: Presented by - Yogesh VyasvictoryvelavaОценок пока нет
- Soft Tissue InjuryДокумент2 страницыSoft Tissue InjuryThiruОценок пока нет
- Motor Functions of Spinal CordДокумент51 страницаMotor Functions of Spinal CordZoafshan Ashfaque100% (1)
- Seizure Disorder, Spinal Injury Neural TumorДокумент52 страницыSeizure Disorder, Spinal Injury Neural TumornipoОценок пока нет
- Anatomy Reviewer 2.0Документ7 страницAnatomy Reviewer 2.0Angeline VegaОценок пока нет
- MusclesДокумент66 страницMusclesusernameОценок пока нет
- Neurology - Saif.wesmosis.2013 104907Документ68 страницNeurology - Saif.wesmosis.2013 104907Helene AlawamiОценок пока нет
- Shoulder InjuryДокумент79 страницShoulder InjurySudipta BhowmickОценок пока нет
- Peripheral CirculationДокумент27 страницPeripheral CirculationRachel ThomsonОценок пока нет
- A Patient's Guide To Radial Tunnel SyndromeДокумент4 страницыA Patient's Guide To Radial Tunnel SyndromeKarunya Vk100% (1)
- Recognising and Classifying Injuries 9c Injuries Recognising ClassifyingДокумент4 страницыRecognising and Classifying Injuries 9c Injuries Recognising ClassifyingJake GarciaОценок пока нет
- Intravenous TherapyДокумент48 страницIntravenous TherapyFrancr ToledanoОценок пока нет
- Postural Assessment (Mia)Документ9 страницPostural Assessment (Mia)im. EliasОценок пока нет
- Bones and Joints TBДокумент19 страницBones and Joints TBmichaelcylОценок пока нет
- Lumbar Disc HerniationДокумент19 страницLumbar Disc HerniationRabie'ahBahananОценок пока нет
- Peripheral Nerve Injury and Repair: Adam Osbourne, 5th Year MedicineДокумент5 страницPeripheral Nerve Injury and Repair: Adam Osbourne, 5th Year Medicineayrahma29Оценок пока нет
- Male GU ExamДокумент5 страницMale GU ExamOmar Farid ElgebalyОценок пока нет
- Anatomy and Pathoanatomic of Lumbosacral PlexusДокумент33 страницыAnatomy and Pathoanatomic of Lumbosacral PlexusRachmad FaisalОценок пока нет
- Nerve Pain and Nerve Damage 2Документ17 страницNerve Pain and Nerve Damage 2Ryan BediОценок пока нет
- Ataxias Neuro Condition DetailedДокумент80 страницAtaxias Neuro Condition DetailedMikail AtiyehОценок пока нет
- Cerebellar StrokeДокумент17 страницCerebellar StrokeAna CotomanОценок пока нет
- Acute Spinal Cord InjuryДокумент3 страницыAcute Spinal Cord InjuryMarisol Dellera ValmoriaОценок пока нет
- DD ScrotumДокумент4 страницыDD ScrotumAy HaanОценок пока нет
- Sequelae of Trumatic Brain InjuryДокумент19 страницSequelae of Trumatic Brain InjuryAnurag SuryawanshiОценок пока нет
- Foot and AnkleДокумент21 страницаFoot and AnkleAli MullaОценок пока нет
- Introduction To Intervertebral Disc Anatomy, Pivd (Lumbar) and Its ManagementДокумент104 страницыIntroduction To Intervertebral Disc Anatomy, Pivd (Lumbar) and Its ManagementVivek SaxenaОценок пока нет
- Neuro-Coordination Umair PTДокумент20 страницNeuro-Coordination Umair PTFatima SeharОценок пока нет
- Joint, Connective Tissue, and Bone Disorders and ManagementДокумент47 страницJoint, Connective Tissue, and Bone Disorders and ManagementAmbreen TariqОценок пока нет
- Neurogenic Bladder: When Nerve Damage Causes Bladder ProblemsДокумент3 страницыNeurogenic Bladder: When Nerve Damage Causes Bladder ProblemsmarselamgeОценок пока нет
- Herniated Disc orДокумент10 страницHerniated Disc orChristine Marie BationОценок пока нет
- What Is PolymyositisДокумент24 страницыWhat Is PolymyositisAshraf MobyОценок пока нет
- Hamstring InjuriesДокумент6 страницHamstring InjuriesIlian GeorgievОценок пока нет
- Budgeting Workshop PowerPointДокумент13 страницBudgeting Workshop PowerPointCj SmithОценок пока нет
- Motor Neuron Disease: Amyotrophic Lateral Sclerosis (ALS)Документ2 страницыMotor Neuron Disease: Amyotrophic Lateral Sclerosis (ALS)james cordenОценок пока нет
- Body Coordination (Mohd Fahim Mohd Farid 4ukm)Документ17 страницBody Coordination (Mohd Fahim Mohd Farid 4ukm)Tham SuperОценок пока нет
- Reflex ExamДокумент4 страницыReflex ExamDan Ali100% (1)
- Check Unit 557 Jan-Feb Genetics v3 PDFДокумент36 страницCheck Unit 557 Jan-Feb Genetics v3 PDFdragon66Оценок пока нет
- Week 1 and 2 PCP Workbook QuestionsДокумент4 страницыWeek 1 and 2 PCP Workbook Questionsapi-479717740100% (1)
- Scapulohumeral PeriarthritisДокумент29 страницScapulohumeral PeriarthritisMárcia PatríciaОценок пока нет
- Ankle Sprain - UpToDateДокумент48 страницAnkle Sprain - UpToDateDavid RyanОценок пока нет
- Week 3 - PCPДокумент3 страницыWeek 3 - PCPapi-479754549100% (1)
- Nerve Compression Syndromes: (Sindroma Jebakan)Документ51 страницаNerve Compression Syndromes: (Sindroma Jebakan)Astri Kartika SariОценок пока нет
- Types of Synovial JointsДокумент7 страницTypes of Synovial Jointsaulia nurfadillahОценок пока нет
- Tuberculosis of Hip JointДокумент25 страницTuberculosis of Hip JointYousra ShaikhОценок пока нет
- PNF FullДокумент46 страницPNF FullHUZAIFA YAMAAN100% (1)
- Clinical Practice GuidelinesДокумент2 страницыClinical Practice GuidelinesEddie WyattОценок пока нет
- Pi Is 0091674906013704Документ2 страницыPi Is 0091674906013704Eddie WyattОценок пока нет
- Pi Is 0091674906013704Документ2 страницыPi Is 0091674906013704Eddie WyattОценок пока нет
- EngДокумент48 страницEngnina nurhayatiОценок пока нет
- Analisis Penetapan Kriteria Kawasan HutanДокумент14 страницAnalisis Penetapan Kriteria Kawasan HutanHarunHasibОценок пока нет
- Jurnal Terapi FaringitisДокумент7 страницJurnal Terapi Faringitisarstantyar0% (1)
- Prophylactic Antipyretics For Prevention of Febrile Seizures Following VaccinationДокумент3 страницыProphylactic Antipyretics For Prevention of Febrile Seizures Following VaccinationEddie WyattОценок пока нет
- Baca Sebelum Instal GameДокумент1 страницаBaca Sebelum Instal GameEddie WyattОценок пока нет
- 59 15-68Документ7 страниц59 15-68Eddie WyattОценок пока нет
- Normal-Pressure Hydrocephalus: Roger SalloumДокумент2 страницыNormal-Pressure Hydrocephalus: Roger SalloumEddie WyattОценок пока нет
- Osteoporosis NOGG Guideline 2017Документ36 страницOsteoporosis NOGG Guideline 2017Claudia Micu100% (1)
- Baca Sebelum Instal GameДокумент1 страницаBaca Sebelum Instal GameEddie WyattОценок пока нет
- Guidline TetanusДокумент363 страницыGuidline TetanusferianaОценок пока нет
- Absensi PraktikumДокумент18 страницAbsensi PraktikumEddie WyattОценок пока нет
- Absensi PraktikumДокумент18 страницAbsensi PraktikumEddie WyattОценок пока нет
- Daftar PustakaДокумент5 страницDaftar PustakaEddie WyattОценок пока нет
- Kumpulan Osce Ukmppd - BimaДокумент2 страницыKumpulan Osce Ukmppd - BimaEddie Wyatt0% (1)
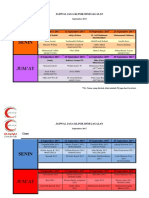
- Jadwal Jaga Klinik Bsmi Jagalan September 2017Документ8 страницJadwal Jaga Klinik Bsmi Jagalan September 2017Eddie WyattОценок пока нет
- Infant Feeding PracticeДокумент46 страницInfant Feeding PracticeEddie WyattОценок пока нет
- Obat BaksosДокумент1 страницаObat BaksosEddie WyattОценок пока нет
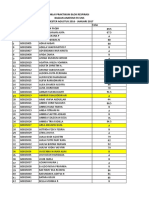
- NIlai 2016Документ31 страницаNIlai 2016Eddie WyattОценок пока нет
- Obat BaksosДокумент1 страницаObat BaksosEddie WyattОценок пока нет
- Zam 7116Документ6 страницZam 7116DdCasadoLasterosОценок пока нет
- Pembahasan Soal UB10 Muskulo 2010Документ10 страницPembahasan Soal UB10 Muskulo 2010Eddie WyattОценок пока нет
- DMS 2014 - B - Basic of Bone & Joint InfectionДокумент28 страницDMS 2014 - B - Basic of Bone & Joint InfectionEddie WyattОценок пока нет
- Jadwal Pembelajaran Laboratorium Anatomi Fakultas Kedokteran UNS IMO 2017Документ1 страницаJadwal Pembelajaran Laboratorium Anatomi Fakultas Kedokteran UNS IMO 2017Eddie WyattОценок пока нет
- Nail Loss: Oleh: Hananto Wildan Habibi (G0014111)Документ11 страницNail Loss: Oleh: Hananto Wildan Habibi (G0014111)Eddie WyattОценок пока нет
- The Fractured Femur: Directed Readings in The ClassroomДокумент68 страницThe Fractured Femur: Directed Readings in The ClassroomEddie Wyatt100% (1)
- TriageДокумент14 страницTriageNiko AndreanОценок пока нет
- Tara Liska ResumeДокумент4 страницыTara Liska Resumeapi-384128955Оценок пока нет
- Rehabilitation Rcpsych Report 2009Документ46 страницRehabilitation Rcpsych Report 2009psychforall100% (2)
- Dental Plans and Rates: Bay AreaДокумент6 страницDental Plans and Rates: Bay AreaJDanaОценок пока нет
- Baclofen KemstroДокумент2 страницыBaclofen KemstroKristi WrayОценок пока нет
- Plugged Milk Ducts and Nipple Blebs: What Are The Symptoms of A Plugged Milk Duct?Документ4 страницыPlugged Milk Ducts and Nipple Blebs: What Are The Symptoms of A Plugged Milk Duct?MuhammadRajifОценок пока нет
- 00 Statistical Report 2016Документ248 страниц00 Statistical Report 2016wudthipanОценок пока нет
- Blood Gases (Abgs) Interpretation Dr/Baha Eldin Hassan Ahmed Fellow Paediatric Critical CareДокумент48 страницBlood Gases (Abgs) Interpretation Dr/Baha Eldin Hassan Ahmed Fellow Paediatric Critical Carehagir alhajОценок пока нет
- Adverse Reaction Blood BankДокумент10 страницAdverse Reaction Blood BankyourfamilydoctorОценок пока нет
- Copd and Cor PulmonalДокумент14 страницCopd and Cor PulmonalAldi RafaelОценок пока нет
- Merchant Shipping (Medicines, Medical Stores and Appliances) Rules, 1994Документ18 страницMerchant Shipping (Medicines, Medical Stores and Appliances) Rules, 1994pravenОценок пока нет
- FUNDA NotesДокумент63 страницыFUNDA NotesNina Anne Paracad0% (1)
- EC2021-Medical Electronics Notes For All Five UnitsДокумент147 страницEC2021-Medical Electronics Notes For All Five UnitsJason Jackson100% (1)
- The Wick: The Magazine of Hartwick College - Summer 2011Документ56 страницThe Wick: The Magazine of Hartwick College - Summer 2011Stephanie BrunettaОценок пока нет
- Hypo ReviewДокумент5 страницHypo ReviewShreyans DamadeОценок пока нет
- ADHDДокумент2 страницыADHDMerijn MattheijssenОценок пока нет
- Trait Theory of PersonalityДокумент5 страницTrait Theory of PersonalityBenitez GheroldОценок пока нет
- GONIOMETRYДокумент6 страницGONIOMETRYchloegmndzОценок пока нет
- PredictiveДокумент7 страницPredictiveAlbert VijayОценок пока нет
- Entire Pharm ClassДокумент173 страницыEntire Pharm ClassnancyОценок пока нет
- CBT OutlineДокумент2 страницыCBT OutlineRoss Laurenne FortunadoОценок пока нет
- Assessing Dehydration in ChildrenДокумент40 страницAssessing Dehydration in ChildrenDr. Jayesh PatidarОценок пока нет
- Fractures of Radius and Ulnar Shaft: Dima HabanjarДокумент56 страницFractures of Radius and Ulnar Shaft: Dima HabanjarDima HabanjarОценок пока нет
- Pediatric Osteomyelitis: Annisa Nur ArifinДокумент18 страницPediatric Osteomyelitis: Annisa Nur ArifinWahyu Adhitya PrawirasatraОценок пока нет
- Metabolic Bone Diseases: Dr. R.C.JindalДокумент73 страницыMetabolic Bone Diseases: Dr. R.C.JindalpriyankОценок пока нет
- Dana Ullman HomeopathyДокумент4 страницыDana Ullman Homeopathydavid_moloneyОценок пока нет
- Bronchodilators and Other Respiratory DrugsДокумент44 страницыBronchodilators and Other Respiratory DrugsastriedamaliaamanatОценок пока нет
- Autism DyslexiaДокумент2 страницыAutism DyslexiaAutismDyslexiaОценок пока нет
- Traumatic Brain Injury PresentationДокумент14 страницTraumatic Brain Injury Presentationapi-413607178Оценок пока нет