Вам также может понравиться
- ImmunologyДокумент103 страницыImmunologyAkila DuraiОценок пока нет
- Rules of Criminal ProcedureДокумент35 страницRules of Criminal ProcedureJames Patrick D. MoralaОценок пока нет
- HyperpituitarismДокумент25 страницHyperpituitarismBheru Lal0% (1)
- EDITED ENDO50items 1Документ12 страницEDITED ENDO50items 1Darren Vargas100% (1)
- Drugs Acting On The Endocrine SystemДокумент58 страницDrugs Acting On The Endocrine SystemAmiel Francisco ReyesОценок пока нет
- Disorders of Endocrine SystemДокумент48 страницDisorders of Endocrine SystemSHARIM ASGHARОценок пока нет
- Cushings Syndrome and Addison Disease - BPTДокумент45 страницCushings Syndrome and Addison Disease - BPTAanchal GuptaОценок пока нет
- Disorders of The Eye LidsДокумент33 страницыDisorders of The Eye Lidsc/risaaq yuusuf ColoowОценок пока нет
- Neoplastic DisordersДокумент36 страницNeoplastic DisordersJSeasharkОценок пока нет
- Nervous TissueДокумент10 страницNervous TissueWrigley PatioОценок пока нет
- Steroids HormonesДокумент15 страницSteroids HormonesZain Ul Abdin Mughal100% (1)
- ANS PharmacologyДокумент68 страницANS PharmacologyAmanuel MaruОценок пока нет
- Cellular Injury and AdaptationsДокумент145 страницCellular Injury and AdaptationsAjmal RockzzОценок пока нет
- Degenerative Diseases of The Nervous SystemДокумент51 страницаDegenerative Diseases of The Nervous SystemJanie-Vi Villamor Ismael-GorospeОценок пока нет
- Urinary Tract InfectionsДокумент6 страницUrinary Tract Infectionspat_tienmin4552Оценок пока нет
- Diseases of Urinary SystemДокумент29 страницDiseases of Urinary SystemHassan.shehri100% (9)
- Parasympathetic Nervous System DrugsДокумент38 страницParasympathetic Nervous System DrugsJon Corpuz AggasidОценок пока нет
- Luteinizing HormoneДокумент8 страницLuteinizing HormoneSaba MalikОценок пока нет
- DiabetesДокумент16 страницDiabetesBabelctgОценок пока нет
- Oestrogen, Progesterone, AndrogensДокумент58 страницOestrogen, Progesterone, AndrogensTandin SonamОценок пока нет
- Sperm Count IncreaseДокумент5 страницSperm Count Increaseomomom2710Оценок пока нет
- Sedative and HypnoticsДокумент26 страницSedative and HypnoticsZarish IftikharОценок пока нет
- Endocrine System: THE Adrenal GlandsДокумент50 страницEndocrine System: THE Adrenal GlandsAbdel Aziz NazihОценок пока нет
- Neoplastic Disease 1Документ69 страницNeoplastic Disease 1Heba IyadОценок пока нет
- SEDATIVE and HYPNOTIC DRUGSДокумент5 страницSEDATIVE and HYPNOTIC DRUGSVaishali Prashar100% (1)
- Chapter 9-SensesДокумент74 страницыChapter 9-SensesMaiah DinglasanОценок пока нет
- Statutory ConstructionДокумент16 страницStatutory ConstructionDash BencioОценок пока нет
- Suprasellar Region PDFДокумент114 страницSuprasellar Region PDFmalex33yОценок пока нет
- Genital Ulcers: DR Hassan M. HusseinДокумент53 страницыGenital Ulcers: DR Hassan M. HusseinPeter Imoje0% (1)
- Fertility and SubfertilityДокумент95 страницFertility and SubfertilitydidiОценок пока нет
- UNIT XIII Drugs Affecting The Reproductive SystemДокумент90 страницUNIT XIII Drugs Affecting The Reproductive Systemrichardmd2100% (1)
- Pituitary Gland: The Master GlandДокумент15 страницPituitary Gland: The Master GlandMohammed ShahanewzОценок пока нет
- About Blood CellsДокумент5 страницAbout Blood CellsJoshua RaviОценок пока нет
- 62 Lecture Menstrual Cycle Abnormalities, Infertility, MenopauseДокумент69 страниц62 Lecture Menstrual Cycle Abnormalities, Infertility, MenopauseTarek TarekОценок пока нет
- PBL 12 - Adrenal GlandsДокумент7 страницPBL 12 - Adrenal GlandsKrishna OochitОценок пока нет
- Drugs Affecting The Female Reproductive SystemДокумент26 страницDrugs Affecting The Female Reproductive SystemAlannes AndalОценок пока нет
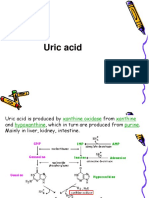
- Uric AcidДокумент30 страницUric AcidKesavanVeeraОценок пока нет
- Genetics Unit OutineДокумент2 страницыGenetics Unit Outinejmunozbio@yahoo.comОценок пока нет
- Atherosclerosis PresentationДокумент90 страницAtherosclerosis PresentationAbu SaifОценок пока нет
- Helicobacter PyloriДокумент33 страницыHelicobacter Pyloritummalapalli venkateswara rao100% (6)
- Cell Communication PDFДокумент109 страницCell Communication PDFediaz_956003100% (1)
- Klinefelter SyndromeДокумент6 страницKlinefelter Syndromemeeeenon100% (1)
- Wound HealingДокумент36 страницWound HealingShahenda El-falkyОценок пока нет
- Cushing SyndromeДокумент8 страницCushing SyndromeArun100% (1)
- Pathology of NeoplasiaДокумент51 страницаPathology of Neoplasiam43Оценок пока нет
- 1st Lecture On The Histology of Female Reproductive System by Dr. RoomiДокумент17 страниц1st Lecture On The Histology of Female Reproductive System by Dr. RoomiMudassar RoomiОценок пока нет
- BIOL 2900 Learning OutcomesДокумент11 страницBIOL 2900 Learning OutcomesTalk To MeОценок пока нет
- N C by Dr. Mohamed Baraka: Ausea AND Vomiting Onstipation AND DiarrheaДокумент72 страницыN C by Dr. Mohamed Baraka: Ausea AND Vomiting Onstipation AND DiarrheaIbrahim Mahmoud AliОценок пока нет
- 1 Epithelial Tissue PDFДокумент104 страницы1 Epithelial Tissue PDFGisela Murdany100% (1)
- Smooth Muscle Physiology by Bushra Akhtar Dhillon (07.04.2020)Документ24 страницыSmooth Muscle Physiology by Bushra Akhtar Dhillon (07.04.2020)Laraib SohailОценок пока нет
- Tall StatureДокумент24 страницыTall StaturedianmutiaОценок пока нет
- DwarfismДокумент5 страницDwarfismjasminemuammilОценок пока нет
- Cushing'S Syndrome: Reported By: Group 4Документ37 страницCushing'S Syndrome: Reported By: Group 4Jovelle AlcantaraОценок пока нет
- Unit 3 Endocrine SystemДокумент36 страницUnit 3 Endocrine SystemdhanashriОценок пока нет
- Type 5 yДокумент4 страницыType 5 yya.prosto.feyОценок пока нет
- EndokrinДокумент27 страницEndokrinSarah Putri AbellysaОценок пока нет
- Cushing's Syndrome, Addison's Disease and Hyperparathyroidism.Документ29 страницCushing's Syndrome, Addison's Disease and Hyperparathyroidism.pranjl100% (1)
- Angeles University Foundation College of Nursing Angeles CityДокумент5 страницAngeles University Foundation College of Nursing Angeles CityCaithlyn KirthleyОценок пока нет
- What Is CushingДокумент10 страницWhat Is CushingkuroroexileОценок пока нет
- NM 24 Endohypothapituit 2007Документ71 страницаNM 24 Endohypothapituit 2007api-26938624Оценок пока нет
- Addisions Disease Alternative Names: Return To TopДокумент9 страницAddisions Disease Alternative Names: Return To TopSuhas IngaleОценок пока нет
- Addison's Disease: Endocrine GlandsДокумент4 страницыAddison's Disease: Endocrine GlandsfynneroОценок пока нет
- The HeartДокумент42 страницыThe HeartJerilee SoCute WattsОценок пока нет
- Digestive SystemДокумент48 страницDigestive SystemJerilee SoCute WattsОценок пока нет
- The Circulatory System-: TransportДокумент13 страницThe Circulatory System-: TransportJerilee SoCute WattsОценок пока нет
- Reproduction and DevelopmentДокумент53 страницыReproduction and DevelopmentJerilee SoCute WattsОценок пока нет
- The Digestive System EssayДокумент3 страницыThe Digestive System EssayJerilee SoCute Watts0% (1)
- The Digestive System: Cont'd (From Swallowing)Документ56 страницThe Digestive System: Cont'd (From Swallowing)Jerilee SoCute WattsОценок пока нет
- Review Questions - HeartДокумент1 страницаReview Questions - HeartJerilee SoCute WattsОценок пока нет
- Lecture 2 Cardiovascular SystemДокумент70 страницLecture 2 Cardiovascular SystemJerilee SoCute WattsОценок пока нет
- Respiratory Centers of The BrainДокумент36 страницRespiratory Centers of The BrainJerilee SoCute WattsОценок пока нет
- Lecture 1 Cardiovascular SystemДокумент70 страницLecture 1 Cardiovascular SystemJerilee SoCute WattsОценок пока нет
- Past Papers Section2Документ13 страницPast Papers Section2Jerilee SoCute Watts50% (2)
- Lymphatic System: Marieb Chapter 20Документ22 страницыLymphatic System: Marieb Chapter 20Jerilee SoCute WattsОценок пока нет
- The Integumentary System: Human Anatomy, 3rd Edition Prentice Hall, © 2001Документ43 страницыThe Integumentary System: Human Anatomy, 3rd Edition Prentice Hall, © 2001Jerilee SoCute WattsОценок пока нет
- Endocrine System: Hormones & HomeostasisДокумент32 страницыEndocrine System: Hormones & HomeostasisJerilee SoCute WattsОценок пока нет
- Endocrine System: Glands & HormonesДокумент78 страницEndocrine System: Glands & HormonesJerilee SoCute WattsОценок пока нет
- Gametogenesis: - Gametes Develop in The Gonads (Sex Cells)Документ12 страницGametogenesis: - Gametes Develop in The Gonads (Sex Cells)Jerilee SoCute WattsОценок пока нет
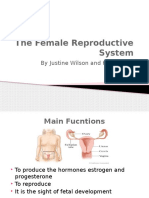
- The Female Reproductive System: by Justine Wilson and Kim IwanskiДокумент18 страницThe Female Reproductive System: by Justine Wilson and Kim IwanskiJerilee SoCute WattsОценок пока нет
- Crypt Orchid Is MДокумент29 страницCrypt Orchid Is Mzackypradana95Оценок пока нет
- Case Studies - Type 1 DiabetesДокумент4 страницыCase Studies - Type 1 Diabeteszenagit1234560% (2)
- Endocrine ClarkДокумент834 страницыEndocrine ClarkKhaled AbdelgalelОценок пока нет
- Study Guide Blood Glucose MonitoringДокумент4 страницыStudy Guide Blood Glucose MonitoringDan Dan ManaoisОценок пока нет
- Association of Empty Sella and Neuroendocrine Disorders in Childhood 1995Документ5 страницAssociation of Empty Sella and Neuroendocrine Disorders in Childhood 1995Paúl Otañez MolinaОценок пока нет
- Secondary Amenorrhea: DR Hanaa AlaniДокумент44 страницыSecondary Amenorrhea: DR Hanaa AlaniAakashОценок пока нет
- Unit 2 Glucose Tolerance TestДокумент10 страницUnit 2 Glucose Tolerance TestMs.V. Mahesha Asst. Prof.Оценок пока нет
- Endocrine System Quiz 1 PDFДокумент6 страницEndocrine System Quiz 1 PDFshasagailОценок пока нет
- Diabetes Mellitus: Specialty Icd 10 Icd 9-Cm Medlineplus Emedicine Patient Uk MeshДокумент2 страницыDiabetes Mellitus: Specialty Icd 10 Icd 9-Cm Medlineplus Emedicine Patient Uk MeshMidaSimamoraОценок пока нет
- Endocrine System - Study NotesДокумент6 страницEndocrine System - Study Notesruchikaydv007Оценок пока нет
- Efek Kombinasi Relaksasi Autogenik Dan Aromaterapi Lavender Terhadap Kadar Glukosa Darah Pada Pasien DM Tipe 2 Tyas Aulia Hanani, Diah RatnawatiДокумент8 страницEfek Kombinasi Relaksasi Autogenik Dan Aromaterapi Lavender Terhadap Kadar Glukosa Darah Pada Pasien DM Tipe 2 Tyas Aulia Hanani, Diah Ratnawatigamma kurnia mahananiОценок пока нет
- Grade 10 3RD Quarter Week 2 Day 12Документ14 страницGrade 10 3RD Quarter Week 2 Day 12Louie Jan SarnoОценок пока нет
- Lyphochek Immunoassay Plus Control Levels 1, 2 and 3: Revision Date 2020-06-29 Indicates Revised InformationДокумент2 страницыLyphochek Immunoassay Plus Control Levels 1, 2 and 3: Revision Date 2020-06-29 Indicates Revised InformationMDD Engineering100% (2)
- LibreView Guide - Italian PaperДокумент12 страницLibreView Guide - Italian PaperJesus MuñozОценок пока нет
- Endocrine GlandsДокумент9 страницEndocrine Glandstadashii100% (1)
- Lab Exercise10 Endocrine SystemДокумент3 страницыLab Exercise10 Endocrine SystemMary Danica MendozaОценок пока нет
- Endocrine System: Related Kidshealth LinksДокумент8 страницEndocrine System: Related Kidshealth LinksDianaCornejoОценок пока нет
- Comment:: Department of Immunology Test Name Result Unit Bio. Ref. Range MethodДокумент1 страницаComment:: Department of Immunology Test Name Result Unit Bio. Ref. Range Methodprakash marimuthuОценок пока нет
- The Endocrinopathies of Anorexia NervosaДокумент13 страницThe Endocrinopathies of Anorexia NervosaCarla MesquitaОценок пока нет
- AIA Specialist Panel ListДокумент7 страницAIA Specialist Panel Listbhavesh10140% (1)
- Thyroid Disease and OsteoporosisДокумент60 страницThyroid Disease and Osteoporosisplay_wright2084Оценок пока нет
- Human Physiology An Integrated Approach 7Th Edition Silverthorn Solutions Manual Full Chapter PDFДокумент36 страницHuman Physiology An Integrated Approach 7Th Edition Silverthorn Solutions Manual Full Chapter PDFcleopatrabanhft1vh7100% (11)
- Chapter 13Документ27 страницChapter 13Itzel XD HerreraОценок пока нет
- NCM 116 Midterm PDFДокумент130 страницNCM 116 Midterm PDFPonciana PasanaОценок пока нет
- Report - WINIE SAKALLEY (231210030217)Документ7 страницReport - WINIE SAKALLEY (231210030217)Winie SakalleyОценок пока нет
- 21 - Adrenal CrisisДокумент5 страниц21 - Adrenal CrisisLenard BangugОценок пока нет
- MTF, Sba-Gmt202: (Ne Osa)Документ5 страницMTF, Sba-Gmt202: (Ne Osa)Zahra HussainОценок пока нет
- Prevalence of Diabetes Mellitus in Patients With AcromegalyДокумент14 страницPrevalence of Diabetes Mellitus in Patients With AcromegalyPunnam Anurag ReddyОценок пока нет