Вам также может понравиться
- GREAnalyticalWritingSupreme 2024 SAMPLEДокумент38 страницGREAnalyticalWritingSupreme 2024 SAMPLEVibrant PublishersОценок пока нет
- Congenital Heart DiseasesДокумент14 страницCongenital Heart DiseasesEulane Ferrer100% (1)
- Legend of The Galactic Heroes, Volume 1 - DawnДокумент273 страницыLegend of The Galactic Heroes, Volume 1 - DawnJon100% (1)
- Agamata Chapter 5Документ10 страницAgamata Chapter 5Drama SubsОценок пока нет
- Garrett-Satan and The Powers (Apocalyptic Vision, Christian Reflection, Baylor University, 2010)Документ8 страницGarrett-Satan and The Powers (Apocalyptic Vision, Christian Reflection, Baylor University, 2010)Luis EchegollenОценок пока нет
- Common Pediatric Fractures: Allyson S. Howe, MD Maj, Usaf, MCДокумент67 страницCommon Pediatric Fractures: Allyson S. Howe, MD Maj, Usaf, MCPrince EdwardОценок пока нет
- Head and Neck ExaminationДокумент25 страницHead and Neck ExaminationDarryl Betts100% (1)
- CH 31 - Assessment and Management of Patients With Vascular Disorders and Problems of PeripheralДокумент16 страницCH 31 - Assessment and Management of Patients With Vascular Disorders and Problems of PeripheralPye Antwan DelvaОценок пока нет
- Fetal Positions and Presentations GuideДокумент11 страницFetal Positions and Presentations GuideShanon France100% (1)
- Rabbit MuscularДокумент5 страницRabbit MuscularJ.D.100% (2)
- Adolescent HealthДокумент19 страницAdolescent Healthhou1212!67% (3)
- Common Drug Stems Cheat SheetДокумент2 страницыCommon Drug Stems Cheat SheetCharis Mae DimaculanganОценок пока нет
- KYLE DE VERA BSA-3A (Auditing & Assurance in SPCL Industries MT Exam) AnswersДокумент3 страницыKYLE DE VERA BSA-3A (Auditing & Assurance in SPCL Industries MT Exam) AnswersKyree Vlade100% (1)
- CH 64 - Management of Patients With Neurologic Infections, Autoimmune Disorders, and NeuropathiesДокумент14 страницCH 64 - Management of Patients With Neurologic Infections, Autoimmune Disorders, and NeuropathiesPye Antwan DelvaОценок пока нет
- SPONSORSHIP GUIDE FOR FIJI'S NATIONAL SPORTS FEDERATIONSДокумент17 страницSPONSORSHIP GUIDE FOR FIJI'S NATIONAL SPORTS FEDERATIONSvaidwara100% (1)
- Abdomen ExaminationДокумент37 страницAbdomen ExaminationJaaydevОценок пока нет
- Microscope Review GuideДокумент34 страницыMicroscope Review GuideWwwanand111100% (1)
- 20764C ENU Companion PDFДокумент192 страницы20764C ENU Companion PDFAllan InurretaОценок пока нет
- Atopic Dermatitis: An Inflammatory Skin DisorderДокумент22 страницыAtopic Dermatitis: An Inflammatory Skin DisorderBonitavanyОценок пока нет
- HESIДокумент29 страницHESIJustin Bunn100% (18)
- COVID 19 ReportДокумент21 страницаCOVID 19 ReportDatu Nor Balindong82% (11)
- Atopic DermatitisДокумент9 страницAtopic DermatitisJorge De VeraОценок пока нет
- Measuring and Describing MotionДокумент22 страницыMeasuring and Describing MotionRenz Dela Cruz ArellanoОценок пока нет
- Coriolis EffectДокумент18 страницCoriolis Effectletter_ashish4444Оценок пока нет
- Final Examination: Polytechnic University of The Philippines Open Universitysysten4Документ1 страницаFinal Examination: Polytechnic University of The Philippines Open Universitysysten4Leigh LynОценок пока нет
- Dy Pac v. Bataan Replevin CaseДокумент2 страницыDy Pac v. Bataan Replevin Caseanalyn100% (1)
- Salas v. First Finance Leasing CorporationДокумент2 страницыSalas v. First Finance Leasing CorporationKatrina PerezОценок пока нет
- Case Study of A Child Age 13 1Документ12 страницCase Study of A Child Age 13 1api-357522475Оценок пока нет
- Skin Barrier Disruption and Filaggrin Mutation PathophysiologyДокумент3 страницыSkin Barrier Disruption and Filaggrin Mutation PathophysiologyBanni Aprilita PratiwiОценок пока нет
- Croup SyndromeДокумент3 страницыCroup SyndromeMabesОценок пока нет
- Phylum RhizopodaДокумент2 страницыPhylum RhizopodaLiborMyslivecek100% (1)
- Ecuadors Restrictive Abortion Laws and Public HealthДокумент21 страницаEcuadors Restrictive Abortion Laws and Public Healthangluna89Оценок пока нет
- Agad V MabatoДокумент3 страницыAgad V MabatoHudson CeeОценок пока нет
- Acceleration in MechanismsДокумент22 страницыAcceleration in Mechanismsadilshahzad2001100% (2)
- Rule 1 BJMP Rule BookДокумент2 страницыRule 1 BJMP Rule BookRudy OrteaОценок пока нет
- Public Speaking Materials and TipsДокумент2 страницыPublic Speaking Materials and Tipsstrawberry_89Оценок пока нет
- Thermodynamics Rankine ExamplesДокумент8 страницThermodynamics Rankine ExamplesSre VinodОценок пока нет
- English 11 SyllabusДокумент3 страницыEnglish 11 SyllabusApricot BlueberryОценок пока нет
- Quiz 07Документ11 страницQuiz 07sullivan583Оценок пока нет
- Pyloric StenosisДокумент11 страницPyloric StenosisJustin CharlesОценок пока нет
- Neutrophils and Asthma: J MonteseirínДокумент15 страницNeutrophils and Asthma: J MonteseirínRupa2811Оценок пока нет
- Cardiovascular DisordersДокумент58 страницCardiovascular Disordersehjing100% (3)
- Debate On Abortion: A Feminist Argument: L. Bishwanth SharmaДокумент6 страницDebate On Abortion: A Feminist Argument: L. Bishwanth SharmaImpact JournalsОценок пока нет
- Quiz 9Документ189 страницQuiz 9Joshua PayneОценок пока нет
- Osce HepatobiliaryДокумент12 страницOsce HepatobiliarySyafinaz AlizainiОценок пока нет
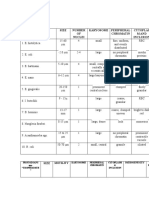
- Table 1: Protozoans Spp. "CYSTS" Size Number OF Nuclei Karyosome Peripheral Chromatin Cytoplas M and InclusionДокумент3 страницыTable 1: Protozoans Spp. "CYSTS" Size Number OF Nuclei Karyosome Peripheral Chromatin Cytoplas M and InclusionJoshua TrinidadОценок пока нет
- Evangelium VitaeДокумент28 страницEvangelium VitaeTobiasОценок пока нет
- Synthesis of Banana Flavor Isoamyl AcetateДокумент12 страницSynthesis of Banana Flavor Isoamyl AcetatePatricia HariramaniОценок пока нет
- Treating Atopic Dermatitis in Children Under 40 CharactersДокумент26 страницTreating Atopic Dermatitis in Children Under 40 CharactersAnnisa SasaОценок пока нет
- Chapter 9 Answer KeyДокумент34 страницыChapter 9 Answer KeyFirebirdGT50% (2)
- Applied Ethics Abortion: 1. Abortion Is An "Act Which A Woman Performs in Voluntarily Terminating, orДокумент8 страницApplied Ethics Abortion: 1. Abortion Is An "Act Which A Woman Performs in Voluntarily Terminating, oryip90Оценок пока нет
- (PHY) 3.02A ElectrocardiogramДокумент10 страниц(PHY) 3.02A ElectrocardiogramMarilou de GuzmanОценок пока нет
- RRLДокумент96 страницRRLKristiene Kyle AquinoОценок пока нет
- Bank Liable for Forgery Despite Contributory NegligenceДокумент13 страницBank Liable for Forgery Despite Contributory NegligenceKirby ReniaОценок пока нет
- Rubrics For PosterДокумент2 страницыRubrics For Posterapi-310947658Оценок пока нет
- Breast Reconstruction With SGAP and IGAP FlapsДокумент9 страницBreast Reconstruction With SGAP and IGAP FlapsJean-Philippe BinderОценок пока нет
- Nanda Nursing Diagnosis Examples:: Vague Uneasy Feeling ofДокумент3 страницыNanda Nursing Diagnosis Examples:: Vague Uneasy Feeling ofYOLANDA P. DELCASTILLOОценок пока нет
- Epicurus Essay On DeathДокумент6 страницEpicurus Essay On DeathKate DickensonОценок пока нет
- The Carnot cycle explainedДокумент3 страницыThe Carnot cycle explainedwaqas_730_2006Оценок пока нет
- Abdominal Wall DefectsДокумент14 страницAbdominal Wall Defectsskeebs23Оценок пока нет
- Steam - Basic Concepts &: FundamentalsДокумент11 страницSteam - Basic Concepts &: FundamentalsermiasОценок пока нет
- Final ArthridesДокумент22 страницыFinal ArthrideskizpirinОценок пока нет
- Rubrics For Writing AssignmentДокумент6 страницRubrics For Writing AssignmentanisahafiszhaZОценок пока нет
- Benign Cystic TeratomaДокумент3 страницыBenign Cystic TeratomaLisa Dwipurnamasari TobingОценок пока нет
- Westmont Bank Ordered to Pay P1.7M for Forgery CaseДокумент3 страницыWestmont Bank Ordered to Pay P1.7M for Forgery CaseMariaFaithFloresFelisartaОценок пока нет
- Case Presentation of a 21-Year-Old Male with Fever and DiarrheaДокумент121 страницаCase Presentation of a 21-Year-Old Male with Fever and DiarrheaErick AncaОценок пока нет
- Chapter 2 Dyspnea-Harrison SummaryДокумент5 страницChapter 2 Dyspnea-Harrison SummaryLeang KarichakОценок пока нет
- Thyroid Status ExaminationДокумент5 страницThyroid Status ExaminationCaliph IVОценок пока нет
- HSBC vs. Cir G.R. No. 166018, June 04, 2014 Facts:: Electronic InstructionsДокумент3 страницыHSBC vs. Cir G.R. No. 166018, June 04, 2014 Facts:: Electronic InstructionsKaren Ryl Lozada BritoОценок пока нет
- Management of Wilms Tumor: Literature Review (NAMA)Документ15 страницManagement of Wilms Tumor: Literature Review (NAMA)DeaNataliaОценок пока нет
- BASIC ACCO Simulated MidtermДокумент10 страницBASIC ACCO Simulated MidtermistepОценок пока нет
- Abdominal Aortic AneurysmДокумент44 страницыAbdominal Aortic Aneurysmalebelucci69Оценок пока нет
- Cardiac Diseases in ChildrenДокумент66 страницCardiac Diseases in ChildrenHarmas Novryan FarezaОценок пока нет
- Odia Tetralogy of FallotДокумент25 страницOdia Tetralogy of Fallotvictorjonathan567Оценок пока нет
- 0 18yrs Child Combined ScheduleДокумент6 страниц0 18yrs Child Combined ScheduleAwal Safar MОценок пока нет
- 0 18yrs Child Combined ScheduleДокумент6 страниц0 18yrs Child Combined ScheduleAwal Safar MОценок пока нет
- Math Practice QuestionsДокумент1 страницаMath Practice QuestionsPye Antwan DelvaОценок пока нет
- Nur2310 GFT 2016-1ref 8855Документ8 страницNur2310 GFT 2016-1ref 8855Pye Antwan DelvaОценок пока нет
- Critical Thinking AckleyДокумент59 страницCritical Thinking AckleyPye Antwan DelvaОценок пока нет
- EENT Disorders StudentsДокумент26 страницEENT Disorders StudentsPye Antwan DelvaОценок пока нет
- AnatomyДокумент90 страницAnatomyPye Antwan DelvaОценок пока нет
- Gi PPTДокумент17 страницGi PPTPye Antwan DelvaОценок пока нет
- London Final Ch38Документ29 страницLondon Final Ch38Pye Antwan DelvaОценок пока нет
- Gu PPTДокумент32 страницыGu PPTPye Antwan DelvaОценок пока нет
- Chapt02 LectureДокумент163 страницыChapt02 LecturePye Antwan DelvaОценок пока нет
- Chapt12 LectureДокумент197 страницChapt12 LecturePye Antwan DelvaОценок пока нет
- Triple TДокумент1 страницаTriple TPye Antwan DelvaОценок пока нет
- Nur1141 Hesi Review 3Документ10 страницNur1141 Hesi Review 3Pye Antwan DelvaОценок пока нет
- Drugs For Men's Health and Reproductive Disorders Ch57 (Student)Документ20 страницDrugs For Men's Health and Reproductive Disorders Ch57 (Student)Pye Antwan DelvaОценок пока нет
- CH 29 - Management of Patients With Structural, Infectious, and Inflmmatory Cardiac DisordersДокумент15 страницCH 29 - Management of Patients With Structural, Infectious, and Inflmmatory Cardiac DisordersPye Antwan Delva100% (1)
- CIHA ch26Документ14 страницCIHA ch26Pye Antwan DelvaОценок пока нет
- PC Pro - October 2016 UKДокумент132 страницыPC Pro - October 2016 UKPye Antwan DelvaОценок пока нет
- CH 29 - Management of Patients With Structural, Infectious, and Inflmmatory Cardiac DisordersДокумент15 страницCH 29 - Management of Patients With Structural, Infectious, and Inflmmatory Cardiac DisordersPye Antwan Delva100% (1)
- Balancing The Cybersecurity BattlefieldДокумент4 страницыBalancing The Cybersecurity BattlefieldLilminowОценок пока нет
- Physics: PAPER 1 Multiple ChoiceДокумент20 страницPhysics: PAPER 1 Multiple Choicelulz.l.n.sОценок пока нет
- Breaking Bad News AssignmentДокумент4 страницыBreaking Bad News AssignmentviksursОценок пока нет
- 11th Commerce Mathematics and Statistics Part II Maharashtra BoardДокумент10 страниц11th Commerce Mathematics and Statistics Part II Maharashtra BoardTanmay Gholap100% (3)
- Chapter 16-Analyzing Qualitative DataДокумент3 страницыChapter 16-Analyzing Qualitative DataLiko Pah TuafОценок пока нет
- FortiEDR Product Overview TrainingДокумент16 страницFortiEDR Product Overview TrainingRafael Steven Soto del CampoОценок пока нет
- Initial Evaluation in The 11th Form B1 LevelДокумент2 страницыInitial Evaluation in The 11th Form B1 LevelDumitru GruscaОценок пока нет
- Case: Macariola Vs AsuncionДокумент18 страницCase: Macariola Vs Asuncionjica GulaОценок пока нет
- Relación Entre Séneca y MaquiaveloДокумент14 страницRelación Entre Séneca y MaquiaveloJuan Pablo TorresОценок пока нет
- Touw 1982 Roses MedievalДокумент14 страницTouw 1982 Roses MedievalВладан СтанковићОценок пока нет
- Sigram Schindler Beteiligungsgesellschaft PetitionДокумент190 страницSigram Schindler Beteiligungsgesellschaft PetitionjoshblackmanОценок пока нет
- Vaclav Havel - From 'Mistake'. SAGEДокумент9 страницVaclav Havel - From 'Mistake'. SAGEADIELruleОценок пока нет
- Coils and InductanceДокумент6 страницCoils and InductanceJoseGarciaRuizОценок пока нет
- Ra 6770Документ8 страницRa 6770Jamiah Obillo HulipasОценок пока нет
- Conquest of The Americas (Eakin-2002)Документ81 страницаConquest of The Americas (Eakin-2002)GregОценок пока нет
- The General RetiresДокумент17 страницThe General Retiresfo100% (1)
- Solución: R T β T R (T) = 1000 Ω ΩДокумент6 страницSolución: R T β T R (T) = 1000 Ω ΩDuvan BayonaОценок пока нет
- Scada Programable Logic Control MCQДокумент2 страницыScada Programable Logic Control MCQAbhigya Bhatnagar85% (13)
- Fuentes CAED PortfolioДокумент32 страницыFuentes CAED PortfoliojsscabatoОценок пока нет
- Automation and Artificial Intelligence in Hospitality and TourismДокумент19 страницAutomation and Artificial Intelligence in Hospitality and TourismShawn WangОценок пока нет
- Activity SheetmagnetismДокумент8 страницActivity SheetmagnetismLey F. Fajutagana100% (1)