Вам также может понравиться
- Precancerous Conditions of Oral CavityДокумент80 страницPrecancerous Conditions of Oral Cavitylarisabrinza12Оценок пока нет
- Presentation 2Документ32 страницыPresentation 2Dr. Bashir MehrОценок пока нет
- ScabiesДокумент39 страницScabiesShahzeb KhanОценок пока нет
- Medicine Lec.11 - HelminthsДокумент39 страницMedicine Lec.11 - Helminths7fefdfbea1Оценок пока нет
- Superficial Mycoses 3Документ8 страницSuperficial Mycoses 3Mohammad KaifОценок пока нет
- Skin in Systemic DiseasesДокумент68 страницSkin in Systemic DiseasesSajin AlexanderОценок пока нет
- Parasitic DiseasesДокумент38 страницParasitic DiseaseslifehuggerОценок пока нет
- Swine DiseasesДокумент28 страницSwine DiseasesTsel KoncetОценок пока нет
- MOST IMPORATANT ONE LINERS Compiled by Medicinosis Magnus 2Документ18 страницMOST IMPORATANT ONE LINERS Compiled by Medicinosis Magnus 2VAIBHAV SHARMA- 122Оценок пока нет
- Hpe Final 110529Документ98 страницHpe Final 110529deeps.u.97Оценок пока нет
- Ectoparasites and Parasites On Human'S Skin/Body Surface: Parasitology DepartmentДокумент36 страницEctoparasites and Parasites On Human'S Skin/Body Surface: Parasitology DepartmentmiaraissaОценок пока нет
- Infancy & Childhood DiseasesДокумент48 страницInfancy & Childhood DiseasesDr. Janarthanan V100% (1)
- Clinical Bacteriology Finals 2.0: Gram Positive BaciliДокумент13 страницClinical Bacteriology Finals 2.0: Gram Positive BaciliEzra LonodОценок пока нет
- Scabies Infection - A Nelson's Series LectureДокумент10 страницScabies Infection - A Nelson's Series LectureRon Christian Neil RodriguezОценок пока нет
- DMS-1 K6 EktoparasitДокумент24 страницыDMS-1 K6 EktoparasitDevina KriskineyaОценок пока нет
- Dermatosa Vesiko BulosaДокумент14 страницDermatosa Vesiko BulosaSyahrul Hamidi NasutionОценок пока нет
- Filariasis: DR Anand Sagar Asst. Prof - Dept. 0f MedicineДокумент29 страницFilariasis: DR Anand Sagar Asst. Prof - Dept. 0f MedicineanandОценок пока нет
- Rabies & FilariasisДокумент29 страницRabies & FilariasisanandОценок пока нет
- Filariasis: DR Anand Sagar Asst. Prof - Dept. 0f MedicineДокумент29 страницFilariasis: DR Anand Sagar Asst. Prof - Dept. 0f MedicineanandОценок пока нет
- Lecture 6 2023Документ16 страницLecture 6 2023ayaessam392002Оценок пока нет
- Ectoparasites and Parasites On Human'S Skin/Body Surface: Parasitology DepartmentДокумент36 страницEctoparasites and Parasites On Human'S Skin/Body Surface: Parasitology DepartmentJimmy Fran IIОценок пока нет
- Salivary Gland DiseaseДокумент18 страницSalivary Gland DiseaseEkky Rizky MaulanaОценок пока нет
- PremalignantДокумент58 страницPremalignantIfabiyi OlaniyiОценок пока нет
- 2019non Limphatic Filaria PДокумент27 страниц2019non Limphatic Filaria PMuhammad Hanif GhifariОценок пока нет
- Benign Neoplasms and HyperplasiasДокумент19 страницBenign Neoplasms and HyperplasiasimperiouxxОценок пока нет
- Cowden S Disease A Rare Cause of Oral Sis 2002 Journal of Laryngology and OtologyДокумент3 страницыCowden S Disease A Rare Cause of Oral Sis 2002 Journal of Laryngology and Otologydasea01Оценок пока нет
- Dermatofitosis FitzpatrickДокумент28 страницDermatofitosis FitzpatrickFadli IlhamОценок пока нет
- Handbook of Skin DiseasesДокумент43 страницыHandbook of Skin DiseasesTrixDelaCruzОценок пока нет
- Pathology of Salivary GlandДокумент27 страницPathology of Salivary GlandkadijaОценок пока нет
- Hydradinitis SupparativaДокумент46 страницHydradinitis SupparativaSaqib SaeedОценок пока нет
- Benign Skin LesionsДокумент109 страницBenign Skin Lesionsrinaldy IX9Оценок пока нет
- Benignskinlesions 141227191914 Conversion Gate01 PDFДокумент109 страницBenignskinlesions 141227191914 Conversion Gate01 PDFrinaldy IX9Оценок пока нет
- Benign Diseases of The Vulvavagina andДокумент58 страницBenign Diseases of The Vulvavagina andHervis FantiniОценок пока нет
- Nematodes LabДокумент57 страницNematodes LabAlaa ZiyadОценок пока нет
- Non Syndromic IcthyosisДокумент109 страницNon Syndromic IcthyosisSRIRAM CKОценок пока нет
- CPC Kurban IIIДокумент173 страницыCPC Kurban IIIkhawar93Оценок пока нет
- Kuliah SMTR VДокумент117 страницKuliah SMTR VHorakhty PrideОценок пока нет
- Dermacase. Pityriasis Rosea.Документ3 страницыDermacase. Pityriasis Rosea.Brenda Ruth PanjaitanОценок пока нет
- Smle Pictorial JunayedДокумент86 страницSmle Pictorial Junayedmonirul islam shohanОценок пока нет
- Chapter 11 Pityriasis Rosea, Pityriasis Rubra Pilaris, and Other Papulosquamous and Hyperkeratotic DiseasesДокумент10 страницChapter 11 Pityriasis Rosea, Pityriasis Rubra Pilaris, and Other Papulosquamous and Hyperkeratotic DiseasesErika KusumawatiОценок пока нет
- 1 StaphylococciДокумент26 страниц1 StaphylococciAyeshaОценок пока нет
- Dermatology OSCE Pictures 1Документ208 страницDermatology OSCE Pictures 1medt80Оценок пока нет
- CandidiasisДокумент51 страницаCandidiasisLincy JohnyОценок пока нет
- Common Cause: Staphylococcus Spp. Streptococcus Spp. Enterococcus SPPДокумент8 страницCommon Cause: Staphylococcus Spp. Streptococcus Spp. Enterococcus SPPAdel mohammadОценок пока нет
- Rashes: Paediatric Dermatology: Ellis HonДокумент95 страницRashes: Paediatric Dermatology: Ellis HonB AuОценок пока нет
- Parasites Associated With Skin Infection - COR TRANXДокумент12 страницParasites Associated With Skin Infection - COR TRANXAna Cristina MontillanoОценок пока нет
- Alimentary Pathology 1 Intro Oral CavityДокумент41 страницаAlimentary Pathology 1 Intro Oral CavityCourtney SandsОценок пока нет
- Referat Kandidosis Kutis - Dhira Dan A. Fari-70700120034 Dan 038Документ14 страницReferat Kandidosis Kutis - Dhira Dan A. Fari-70700120034 Dan 038Ahmad Fari Arief LopaОценок пока нет
- Diagnosis of Conjuctivitis: Ahsan Ali ROLL NO: 260Документ9 страницDiagnosis of Conjuctivitis: Ahsan Ali ROLL NO: 260Farhan AfzalОценок пока нет
- Diagnosis and Treatment of The Disorders of PigsДокумент409 страницDiagnosis and Treatment of The Disorders of PigsStevanОценок пока нет
- Skin PathologyДокумент42 страницыSkin PathologykateОценок пока нет
- Fungal Infections-MlcДокумент31 страницаFungal Infections-Mlcsamuel gathenyaОценок пока нет
- Dracunculus Medinensis: SynonymsДокумент24 страницыDracunculus Medinensis: SynonymsFatemaОценок пока нет
- Pathology Assignment (Aflatoxicosis, Aspergillosis, Candidiasis, Coccidiosis, Degnala, Rabies)Документ5 страницPathology Assignment (Aflatoxicosis, Aspergillosis, Candidiasis, Coccidiosis, Degnala, Rabies)Suraj_SubediОценок пока нет
- Lesson 8 PEDICULOSISДокумент39 страницLesson 8 PEDICULOSISJulius Memeg PanayoОценок пока нет
- Harper's Textbook of Pediatric DermatologyОт EverandHarper's Textbook of Pediatric DermatologyProf. Dr. Alan D. IrvineОценок пока нет
- Gram Negative CocciДокумент21 страницаGram Negative CocciAyeshaОценок пока нет
- Sqweqwesf Erwrewfsdfs Adasd Dhe: Dermnet NZДокумент19 страницSqweqwesf Erwrewfsdfs Adasd Dhe: Dermnet NZkdwazirОценок пока нет
- Pityriasis Versicolor: Superficial Malassezia FurfurДокумент10 страницPityriasis Versicolor: Superficial Malassezia FurfurMafie BarreiroОценок пока нет
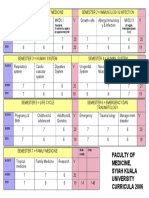
- Faculty of Medicine, Syiah Kuala University Curricula 2006Документ1 страницаFaculty of Medicine, Syiah Kuala University Curricula 2006wirdahajaОценок пока нет
- TOEFL TEST Dan Kunci JawabanДокумент5 страницTOEFL TEST Dan Kunci JawabanwirdahajaОценок пока нет
- Tinea UnguiumДокумент8 страницTinea UnguiumwirdahajaОценок пока нет
- Metabolic EncephalopathyДокумент26 страницMetabolic Encephalopathywirdahaja100% (3)
- Anatomy of The Ear HearingДокумент14 страницAnatomy of The Ear HearingwirdahajaОценок пока нет
- Fever and RashДокумент14 страницFever and RashwirdahajaОценок пока нет
- Defense Mechanism (IB)Документ60 страницDefense Mechanism (IB)wirdahajaОценок пока нет
- Follow Up: No Tanggal Subjektif Objektif Assessment Planning TerapiДокумент4 страницыFollow Up: No Tanggal Subjektif Objektif Assessment Planning TerapiwirdahajaОценок пока нет
- Clinical PathwayДокумент154 страницыClinical Pathwaywirdahaja100% (1)
- AISOY1 KiK User ManualДокумент28 страницAISOY1 KiK User ManualLums TalyerОценок пока нет
- Continuing Professional Development PlanДокумент4 страницыContinuing Professional Development Planvviki50% (2)
- Volvo BL 71 ManualДокумент280 страницVolvo BL 71 ManualAlberto G.D.100% (2)
- NHD Process PaperДокумент2 страницыNHD Process Paperapi-203024952100% (1)
- Diogenes Laertius-Book 10 - Epicurus - Tomado de Lives of The Eminent Philosophers (Oxford, 2018) PDFДокумент54 страницыDiogenes Laertius-Book 10 - Epicurus - Tomado de Lives of The Eminent Philosophers (Oxford, 2018) PDFAndres Felipe Pineda JaimesОценок пока нет
- Hanwha Q Cells Data Sheet Qpeak L-g4.2 360-370 2017-10 Rev02 NaДокумент2 страницыHanwha Q Cells Data Sheet Qpeak L-g4.2 360-370 2017-10 Rev02 NazulfikarОценок пока нет
- FHWA Guidance For Load Rating Evaluation of Gusset Plates in Truss BridgesДокумент6 страницFHWA Guidance For Load Rating Evaluation of Gusset Plates in Truss BridgesPatrick Saint-LouisОценок пока нет
- Ateneo de Manila University: Submitted byДокумент5 страницAteneo de Manila University: Submitted byCuster CoОценок пока нет
- Total Physical Response (G4)Документ3 страницыTotal Physical Response (G4)Aq Nadzrul LarhОценок пока нет
- Leadership and Management in Different Arts FieldsДокумент10 страницLeadership and Management in Different Arts Fieldsjay jayОценок пока нет
- Img 20201010 0005Документ1 страницаImg 20201010 0005Tarek SalehОценок пока нет
- Ej. 1 Fin CorpДокумент3 страницыEj. 1 Fin CorpChantal AvilesОценок пока нет
- Geotechnical PaperДокумент16 страницGeotechnical PaperTxavo HesiarenОценок пока нет
- 2500 Valve BrochureДокумент12 страниц2500 Valve BrochureJurie_sk3608Оценок пока нет
- Full Project LibraryДокумент77 страницFull Project LibraryChala Geta0% (1)
- Arithmetic QuestionsДокумент2 страницыArithmetic QuestionsAmir KhanОценок пока нет
- CII Sohrabji Godrej GreenДокумент30 страницCII Sohrabji Godrej GreenRITHANYAA100% (2)
- FMEA Minus The PainДокумент7 страницFMEA Minus The PainMUNISОценок пока нет
- Caring For Women Experiencing Breast Engorgement A Case ReportДокумент6 страницCaring For Women Experiencing Breast Engorgement A Case ReportHENIОценок пока нет
- Lesson 1 3 Transes in Reading in Philippine HistoryДокумент17 страницLesson 1 3 Transes in Reading in Philippine HistoryNAPHTALI WILLIAMS GOОценок пока нет
- A Literature Review of Retailing Sector and BusineДокумент21 страницаA Literature Review of Retailing Sector and BusineSid MichaelОценок пока нет
- Based On PSA 700 Revised - The Independent Auditor's Report On A Complete Set of General Purpose Financial StatementsДокумент12 страницBased On PSA 700 Revised - The Independent Auditor's Report On A Complete Set of General Purpose Financial Statementsbobo kaОценок пока нет
- Gis Data Creation in Bih: Digital Topographic Maps For Bosnia and HerzegovinaДокумент9 страницGis Data Creation in Bih: Digital Topographic Maps For Bosnia and HerzegovinaGrantОценок пока нет
- Imabalacat DocuДокумент114 страницImabalacat DocuJänrëýMåmårìlSälängsàngОценок пока нет
- John DrydenДокумент3 страницыJohn DrydenDunas SvetlanaОценок пока нет
- Quality Control of Rigid Pavements 1Документ58 страницQuality Control of Rigid Pavements 1pranjpatil100% (1)
- LP32HS User Manual v1Документ52 страницыLP32HS User Manual v1tonizx7rrОценок пока нет
- Create A Visual DopplerДокумент1 страницаCreate A Visual DopplerRahul GandhiОценок пока нет
- CISF Manual Final OriginalДокумент17 страницCISF Manual Final OriginalVaishnavi JayakumarОценок пока нет
- CHAPTER IV The PSYCHOLOGY of YOGA Yoga, One Among The Six Orthodox Schools of Indian ... (PDFDrive)Документ64 страницыCHAPTER IV The PSYCHOLOGY of YOGA Yoga, One Among The Six Orthodox Schools of Indian ... (PDFDrive)kriti madhokОценок пока нет