Вам также может понравиться
- Hearing AidДокумент4 страницыHearing AiddnllkzaОценок пока нет
- Hearing Aids FinalДокумент9 страницHearing Aids FinalVishal GauravОценок пока нет
- Your Guide To Hearing AidsДокумент20 страницYour Guide To Hearing AidsMarhama FitrianiОценок пока нет
- EDE101-Hearing AidsДокумент5 страницEDE101-Hearing AidsΑнмєɒ FσυαɒОценок пока нет
- Hearing Aids: What Is A Hearing Aid?Документ6 страницHearing Aids: What Is A Hearing Aid?Alfeus GradyОценок пока нет
- Hearing Aids: What Is A Hearing Aid?Документ6 страницHearing Aids: What Is A Hearing Aid?ritaamirОценок пока нет
- Assistive Listening DevicesДокумент8 страницAssistive Listening DevicesJenny Rose PamatОценок пока нет
- CNS PBL 7Документ8 страницCNS PBL 7Hugh JacobsОценок пока нет
- Middle Ear ImplantsДокумент23 страницыMiddle Ear ImplantsShilpa RbОценок пока нет
- Listening With Our Teeth! The Soundbite Hearing Aid: A New Technology For Single-Sided DeafnessДокумент2 страницыListening With Our Teeth! The Soundbite Hearing Aid: A New Technology For Single-Sided Deafnessはじめ ましてОценок пока нет
- Types of Hearing LossДокумент42 страницыTypes of Hearing LossKesuma Larasati0% (1)
- 9 Audiometer 03 07 2023Документ30 страниц9 Audiometer 03 07 2023Kushagra Narang 21BML0031Оценок пока нет
- Hearing AidsДокумент13 страницHearing AidsHarsh GuptaОценок пока нет
- Environmental Health and Safety University of TennesseeДокумент63 страницыEnvironmental Health and Safety University of Tennesseeimran_istОценок пока нет
- Electronic Stethoscope: Kushagra Bhatheja Ravi Shankar Davinder Singh Ece Ii Eceii Enroll No.-1461502807 Enroll No.Документ4 страницыElectronic Stethoscope: Kushagra Bhatheja Ravi Shankar Davinder Singh Ece Ii Eceii Enroll No.-1461502807 Enroll No.ucantseeme0000Оценок пока нет
- AUDIOMETERДокумент55 страницAUDIOMETERANUSAYA SAHUОценок пока нет
- AssistiveDevices 508Документ6 страницAssistiveDevices 508Галя ЦаневаОценок пока нет
- Hearing Conservation: Trina Redford, Industrial HygienistДокумент34 страницыHearing Conservation: Trina Redford, Industrial HygienistNOrsaodah ZInОценок пока нет
- jpg20005 1215 1215Документ1 страницаjpg20005 1215 1215Rahma R SОценок пока нет
- Hearing Aid PPT BaruДокумент21 страницаHearing Aid PPT BaruJimmy AnwarОценок пока нет
- Ultrasonic Directive SpeakerДокумент42 страницыUltrasonic Directive SpeakerNakul NemaОценок пока нет
- Welcome You All: BY:lokendra YadavДокумент32 страницыWelcome You All: BY:lokendra YadavLokender YadavОценок пока нет
- So,You Want To Be An Audio Engineer: A Complete Beginners Guide For Selecting Audio GearОт EverandSo,You Want To Be An Audio Engineer: A Complete Beginners Guide For Selecting Audio GearРейтинг: 5 из 5 звезд5/5 (1)
- Aspects of Hearing Aids Fitting ProceduresДокумент150 страницAspects of Hearing Aids Fitting ProceduresakОценок пока нет
- DSP 3rd YearДокумент36 страницDSP 3rd YearAgripino Verdera Jr.Оценок пока нет
- CPD - Public Address SystemДокумент93 страницыCPD - Public Address SystemThilina SarangaОценок пока нет
- Noise Pollution For Environmental ScienceДокумент12 страницNoise Pollution For Environmental Scienceobaid kuraishyОценок пока нет
- Hearing Aids and Assistive TechnologiesДокумент3 страницыHearing Aids and Assistive Technologiesapi-300459905Оценок пока нет
- Latest To Hearing Amp TechnolgiesДокумент22 страницыLatest To Hearing Amp Technolgiesapi-349133705Оценок пока нет
- FPGA Based Signal Processing Implementation For Hearing ImpairmentДокумент5 страницFPGA Based Signal Processing Implementation For Hearing ImpairmentGrimmjow JaegerjaquezОценок пока нет
- Environmental Health and Safety University of TennesseeДокумент54 страницыEnvironmental Health and Safety University of TennesseeEm WaОценок пока нет
- Hearing Conservation Training: Environmental Health and Safety University of TennesseeДокумент54 страницыHearing Conservation Training: Environmental Health and Safety University of TennesseeMG NandanОценок пока нет
- Killlionetal 2016 Hearing Aid Transducers Chapter Killion Van Halteren Stenfelt WarrenДокумент35 страницKilllionetal 2016 Hearing Aid Transducers Chapter Killion Van Halteren Stenfelt Warrenbuitruongphat.workОценок пока нет
- Biomedical Instrumentation Tic 701 Bmi-Unit-4-5Документ40 страницBiomedical Instrumentation Tic 701 Bmi-Unit-4-5bhardwejanujОценок пока нет
- Branch - Electronics ID No - 16EL035 Name - Utsav Fuletra Subject - Seminar Semester - 7 Year - 4 Mentors - Ajay Daiya and Mahendra PrajapatiДокумент27 страницBranch - Electronics ID No - 16EL035 Name - Utsav Fuletra Subject - Seminar Semester - 7 Year - 4 Mentors - Ajay Daiya and Mahendra PrajapatiUtsav100% (1)
- Tugas Nursing FixДокумент4 страницыTugas Nursing FixCazorlaОценок пока нет
- Characteristic of HeadphoneДокумент7 страницCharacteristic of HeadphoneAli RazaОценок пока нет
- The Underlying In-Ear Headphone Protection Article PostДокумент4 страницыThe Underlying In-Ear Headphone Protection Article Postsauce13mondayОценок пока нет
- Rehab Tech21Документ114 страницRehab Tech21Appas SahaОценок пока нет
- Cochlear Implants As Hearing Aid in Auditory Systems: Ei-5112 Modern Biomedical InstrumentationДокумент14 страницCochlear Implants As Hearing Aid in Auditory Systems: Ei-5112 Modern Biomedical InstrumentationPradeep76448Оценок пока нет
- Environmental Science 2 - 12 Noise PollutionДокумент9 страницEnvironmental Science 2 - 12 Noise Pollutionrayan ashrafОценок пока нет
- 3-01045-s Spectralresolution-SpДокумент6 страниц3-01045-s Spectralresolution-Spapi-260192872Оценок пока нет
- Hearing AidsДокумент20 страницHearing Aidssathsh kumarОценок пока нет
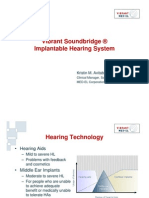
- Vibrant Soundbridge ® Implantable Hearing System: Kristin M. Avitabile, MS, CCC-AДокумент35 страницVibrant Soundbridge ® Implantable Hearing System: Kristin M. Avitabile, MS, CCC-AsemiragaОценок пока нет
- Dr. Atul Jain - Ear SurgeryДокумент36 страницDr. Atul Jain - Ear SurgeryPushpanjali Crosslay HospitalОценок пока нет
- Middle Ear ImplantsДокумент5 страницMiddle Ear ImplantsPrakashОценок пока нет
- Noise PollutionДокумент35 страницNoise PollutionNikhil WaghОценок пока нет
- Physiologic Response To Noise and VibrationДокумент86 страницPhysiologic Response To Noise and VibrationEly-Carla Marshall100% (1)
- Cochlear ImplantationДокумент33 страницыCochlear ImplantationRohit SinghalОценок пока нет
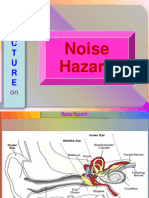
- Noise HazardДокумент20 страницNoise HazardRicky jhonsОценок пока нет
- Surgical Rehabilitation of Deafness With Partially Implantable Hearing Aid Using Piezoelectric Ceramic Bimorpli Ossicular VibratorДокумент8 страницSurgical Rehabilitation of Deafness With Partially Implantable Hearing Aid Using Piezoelectric Ceramic Bimorpli Ossicular Vibratorİsmail KahramanОценок пока нет
- Human Performance 1. 5 EarДокумент60 страницHuman Performance 1. 5 EarelenavarrojosefrОценок пока нет
- External Ear: Consists of Pinna and The External Auditory Meatus Up To The Lateral Border of The Tympanic MembraneДокумент14 страницExternal Ear: Consists of Pinna and The External Auditory Meatus Up To The Lateral Border of The Tympanic MembraneJiten MavОценок пока нет
- Cochlear ImplantДокумент33 страницыCochlear ImplantNithiyah DevarajuОценок пока нет
- ClassДокумент20 страницClassmeeturammuОценок пока нет
- Audio SpotДокумент3 страницыAudio SpotRohinikatkadeОценок пока нет
- Hasil Stok Opname Des 2018Документ55 страницHasil Stok Opname Des 2018Arif Nugroho SetiawanОценок пока нет
- No. Nama Barang: Harga BeliДокумент4 страницыNo. Nama Barang: Harga BeliArif Nugroho SetiawanОценок пока нет
- Bells Palsy Slides 070214Документ50 страницBells Palsy Slides 070214Arif Nugroho SetiawanОценок пока нет
- Acoustic Neuroma Acoustic Neuroma & Hearing LossДокумент47 страницAcoustic Neuroma Acoustic Neuroma & Hearing LossArif Nugroho SetiawanОценок пока нет
- 1 - Geriatric Assessment - An Office-Based ApproachДокумент13 страниц1 - Geriatric Assessment - An Office-Based ApproachMac NoonОценок пока нет
- My Choice of Gallaudet UniversityДокумент3 страницыMy Choice of Gallaudet Universityvidur_talrejaОценок пока нет
- Ear Training Essentials PDFДокумент85 страницEar Training Essentials PDFGuillermo Nava67% (3)
- CEHH Issue 20 - Noise-Induced Hearing LossДокумент12 страницCEHH Issue 20 - Noise-Induced Hearing LossYaumil ChoiriОценок пока нет
- Case StudyДокумент9 страницCase StudyDevashish Sajwan100% (1)
- Hazard 16 NoiseДокумент1 страницаHazard 16 NoisecerajibОценок пока нет
- Occupational Health Hazards Due To Mine Dust: Unit-14Документ9 страницOccupational Health Hazards Due To Mine Dust: Unit-14Dinesh dhakarОценок пока нет
- Deaf Culture Presentation-Brady-Angie-KaylaДокумент13 страницDeaf Culture Presentation-Brady-Angie-Kaylaapi-436090845100% (1)
- Tinnitus Today June 1989 Vol 14, No 2Документ20 страницTinnitus Today June 1989 Vol 14, No 2American Tinnitus AssociationОценок пока нет
- 300+ TOP Special Education MCQs and Answers Quiz Exam 2024Документ68 страниц300+ TOP Special Education MCQs and Answers Quiz Exam 2024broadfiberkpr100% (1)
- Project NewДокумент33 страницыProject Newceeyem83% (12)
- Management Strategies For Multiple Handicap ChildrenДокумент22 страницыManagement Strategies For Multiple Handicap ChildrenPreeti SinghОценок пока нет
- Letter On ASL at Wootton GraduationДокумент2 страницыLetter On ASL at Wootton GraduationParents' Coalition of Montgomery County, MarylandОценок пока нет
- Everyday English Book 1 c1902Документ525 страницEveryday English Book 1 c1902Anurag Goel0% (1)
- Guide To Speech AudiometryДокумент16 страницGuide To Speech Audiometrywaleed yehiaОценок пока нет
- The Vision S S 18 PsychotropicalДокумент21 страницаThe Vision S S 18 PsychotropicalHimali Lalwani40% (5)
- Chapter 9 Sound WavesДокумент28 страницChapter 9 Sound WavesDom Christian LastОценок пока нет
- Suddenly Installed Idiopathic Hearing LossДокумент16 страницSuddenly Installed Idiopathic Hearing LossSimina ÎntunericОценок пока нет
- Professional Poisoning With Toxic GasesДокумент78 страницProfessional Poisoning With Toxic GasesAnonymous JMnKM6KrОценок пока нет
- Comaparative Education (6466) ASS#2Документ28 страницComaparative Education (6466) ASS#2anam ashrafОценок пока нет
- 13.dysconscious Audism-Genie GertzДокумент10 страниц13.dysconscious Audism-Genie Gertzאדמטהאוצ'והОценок пока нет
- Language of Early-And Later-Identified Children With Hearing LossДокумент13 страницLanguage of Early-And Later-Identified Children With Hearing LossRonald Ivan WijayaОценок пока нет
- Sed341 - Marse RulesДокумент7 страницSed341 - Marse Rulesapi-601576557Оценок пока нет
- Taxi Accessibility ChecklistДокумент2 страницыTaxi Accessibility ChecklistIRUОценок пока нет
- Fbs Lesson Plan 2Документ6 страницFbs Lesson Plan 2Joday67% (3)
- Get Set Skills Employment Training Model For PracticeДокумент50 страницGet Set Skills Employment Training Model For PracticeIsabelОценок пока нет
- Jurnal THT NiaДокумент5 страницJurnal THT NianiajaplaniОценок пока нет
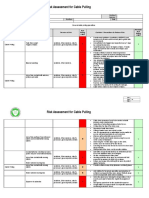
- Cable PullingДокумент4 страницыCable Pullingmykelrenz90% (10)
- Smart Hand Glove Translation For DeafДокумент5 страницSmart Hand Glove Translation For DeafAmazing videos0% (1)
- OshaДокумент42 страницыOshaImran DDzОценок пока нет