Вам также может понравиться
- Care of Patients With CastДокумент2 страницыCare of Patients With CastIan RamaОценок пока нет
- Traction & Application of p0pДокумент19 страницTraction & Application of p0pSham NazrinОценок пока нет
- Geriatric RehabilitationДокумент16 страницGeriatric RehabilitationAjay DherwaniОценок пока нет
- Amputation: by Ashenafi Zemed MSC PTДокумент25 страницAmputation: by Ashenafi Zemed MSC PTHęñøķ BęŕhãñęОценок пока нет
- 4th Year MBBS Question Papers RGUHS OrthopaedicsДокумент22 страницы4th Year MBBS Question Papers RGUHS OrthopaedicsBikram HaldarОценок пока нет
- 3rd Coxa Vara ValgaДокумент30 страниц3rd Coxa Vara ValgaMandar printОценок пока нет
- Fracture in ChildrenДокумент40 страницFracture in ChildrenMutiara Jihad100% (1)
- Amputation: Dr. Abdul Rashad Senior Lecturer DPT, Mphill (Opt), Mppta United College of Physical TherapyДокумент31 страницаAmputation: Dr. Abdul Rashad Senior Lecturer DPT, Mphill (Opt), Mppta United College of Physical Therapypasha100% (1)
- Family Welfare Program & Population PolicyДокумент56 страницFamily Welfare Program & Population PolicyNirmalya SinhaОценок пока нет
- Para PhimosisДокумент9 страницPara PhimosisNazurah Azmira100% (1)
- Fractures: Mary Grace B. Gutierrez Resti Mariano Ma. Cindy O. BautistaДокумент50 страницFractures: Mary Grace B. Gutierrez Resti Mariano Ma. Cindy O. BautistaJustin Ahorro-DionisioОценок пока нет
- SC - Fracture ZMHДокумент51 страницаSC - Fracture ZMHMis StromОценок пока нет
- Case Presentation VijayДокумент33 страницыCase Presentation VijayRaghu NadhОценок пока нет
- Principle of Fracture ManagementДокумент15 страницPrinciple of Fracture ManagementBabyprincess OoiОценок пока нет
- Barium Studies: Presented byДокумент18 страницBarium Studies: Presented byHannah samuelОценок пока нет
- External Fixation: Nursing Best Practice GuidelinesДокумент25 страницExternal Fixation: Nursing Best Practice GuidelinesDoneva Lyn MedinaОценок пока нет
- Cast and TractionsДокумент12 страницCast and TractionsNoemi Nazareno MarceloОценок пока нет
- Tuberculosis of SpineДокумент11 страницTuberculosis of SpineSepti RahadianОценок пока нет
- LaryngoscopeДокумент15 страницLaryngoscopeIhteshamОценок пока нет
- Adolescent Girls Anaemia Control ProgramДокумент38 страницAdolescent Girls Anaemia Control ProgramKarunya VkОценок пока нет
- NeuroblastomaДокумент33 страницыNeuroblastomahariОценок пока нет
- 6 Minute Walk Test InstructionsДокумент6 страниц6 Minute Walk Test InstructionscpradheepОценок пока нет
- Vitiligo PPT (1) .PPTX LectureДокумент35 страницVitiligo PPT (1) .PPTX LectureVinay DhranaОценок пока нет
- Blood Supply of BrainДокумент2 страницыBlood Supply of BrainvmagtotoОценок пока нет
- Amputation: Sites of Amputation: UEДокумент6 страницAmputation: Sites of Amputation: UEChristine PilarОценок пока нет
- Anemia: Presented byДокумент36 страницAnemia: Presented byParmvir Singh100% (1)
- HYDROCEPHALUSДокумент63 страницыHYDROCEPHALUSAjeng Aristiany Rahawarin100% (2)
- Spinal TuberculosisДокумент46 страницSpinal TuberculosisAbby Austero100% (1)
- Cardiorespiratory AssessmentДокумент7 страницCardiorespiratory AssessmentmalarvelykОценок пока нет
- Operation Theatre EvaluationДокумент1 страницаOperation Theatre EvaluationshivaОценок пока нет
- Dissertation Submitted To: The Tamil Nadu Dr.M.G.R.Medical UniversityДокумент13 страницDissertation Submitted To: The Tamil Nadu Dr.M.G.R.Medical UniversityHenry Manuel PrinceОценок пока нет
- A Cross Sectional Study To Assess The Knowledge, Attitude and Practice Towards Road SafetyДокумент11 страницA Cross Sectional Study To Assess The Knowledge, Attitude and Practice Towards Road SafetycksОценок пока нет
- CTEVДокумент61 страницаCTEVSylvia LoongОценок пока нет
- Degenerative Spinal DisordersДокумент47 страницDegenerative Spinal Disordersasad1912Оценок пока нет
- Open Jejunostomy: Steven J. Hughes, MD and A. James Moser, MDДокумент8 страницOpen Jejunostomy: Steven J. Hughes, MD and A. James Moser, MDAndres BernalОценок пока нет
- Congenital Dysplasia of Hip (CDH) Developmental Dysplasia of The Hip (DDH)Документ50 страницCongenital Dysplasia of Hip (CDH) Developmental Dysplasia of The Hip (DDH)NarishaAmeliaОценок пока нет
- Orthopedic EquipmentsДокумент14 страницOrthopedic Equipmentsdavid_soОценок пока нет
- Antepartum Haemorrhage: BY: Ms. R. Liangkiuwiliu Assistant Professor, Obg SSNSR, SuДокумент44 страницыAntepartum Haemorrhage: BY: Ms. R. Liangkiuwiliu Assistant Professor, Obg SSNSR, SuLiangkiuwiliuОценок пока нет
- StrokeДокумент6 страницStrokeRaulLopezJaimeОценок пока нет
- Herpes ZosterДокумент16 страницHerpes ZosterColleen De la RosaОценок пока нет
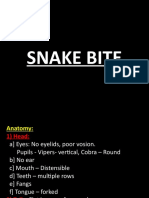
- Snake BiteДокумент61 страницаSnake Biteniraj_sdОценок пока нет
- Pediatric OrthopaedicДокумент66 страницPediatric OrthopaedicDhito RodriguezОценок пока нет
- Basic Principles of Surgery: DEVELOPING A SURGICAL DIAGNOSIS: Important DecisionsДокумент5 страницBasic Principles of Surgery: DEVELOPING A SURGICAL DIAGNOSIS: Important DecisionsStudent FemОценок пока нет
- Metabolic Bone DisordersДокумент24 страницыMetabolic Bone Disordersbpt20% (1)
- HypothyroidismДокумент54 страницыHypothyroidismagakshat23Оценок пока нет
- Urinary Tract ObstructionДокумент56 страницUrinary Tract ObstructionMicky FantaОценок пока нет
- 4-Conservative Treatment FX, CastingДокумент53 страницы4-Conservative Treatment FX, CastingMuhammad TaqwaОценок пока нет
- Indirani College of Nursing: AmputationДокумент7 страницIndirani College of Nursing: AmputationdhanasundariОценок пока нет
- 1 - General Complications of Fractures - d3Документ27 страниц1 - General Complications of Fractures - d3Jheng-Dao Yang100% (1)
- Pelvic Fractures ManagementДокумент24 страницыPelvic Fractures ManagementSerenna DehalooОценок пока нет
- Future Challenges in Physical TherapyДокумент9 страницFuture Challenges in Physical TherapyIqra KanwalОценок пока нет
- Amputation AssignmentДокумент19 страницAmputation Assignmentmushimiyimana jacquelineОценок пока нет
- Geriatric RehabilitationДокумент31 страницаGeriatric RehabilitationsmrutiptОценок пока нет
- Application and Care of Cryo Cuff 1Документ13 страницApplication and Care of Cryo Cuff 1susie eusebius mudi100% (1)
- Muscle Re-EducationДокумент41 страницаMuscle Re-EducationS.JAIVIGNESH OTОценок пока нет
- 2023 OB/GYN Coding Manual: Components of Correct CodingОт Everand2023 OB/GYN Coding Manual: Components of Correct CodingОценок пока нет
- Practical Gastroenterology and Hepatology Board Review ToolkitОт EverandPractical Gastroenterology and Hepatology Board Review ToolkitKenneth R. DeVaultОценок пока нет
- Disseminated Intravascular Coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandDisseminated Intravascular Coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- NBCE Acupuncture Exam Review NotesДокумент77 страницNBCE Acupuncture Exam Review Notesdarbyje100% (8)
- Newborn Nursery Observation SheetДокумент7 страницNewborn Nursery Observation SheetCynthia Gail HeathОценок пока нет
- Upper Limb Set 1Документ6 страницUpper Limb Set 1Zain RehmanОценок пока нет
- 10752-02 CH02 Final PDFДокумент28 страниц10752-02 CH02 Final PDFDejan MilenkovicОценок пока нет
- Bettencourt Chikung Standing Like A TreeДокумент13 страницBettencourt Chikung Standing Like A TreepsetoОценок пока нет
- Surgeon's KnotДокумент2 страницыSurgeon's KnotSanjay PrakashОценок пока нет
- Joint Mobilization - Upper ExtremityДокумент11 страницJoint Mobilization - Upper ExtremityRicha Mahajan50% (2)
- Dress Form: ARM Make AДокумент6 страницDress Form: ARM Make AamelieОценок пока нет
- Elbow and Sport 1st Ed (BUKU)Документ263 страницыElbow and Sport 1st Ed (BUKU)Tri Waluyo100% (1)
- YOGIC SUKSMA VYAYAMA Dhirendra Brahmacharya PDFДокумент75 страницYOGIC SUKSMA VYAYAMA Dhirendra Brahmacharya PDFMaggie MaviОценок пока нет
- Shahal - CASE STUDY (1) - 230321 - 133348Документ46 страницShahal - CASE STUDY (1) - 230321 - 133348shauryashettigarОценок пока нет
- MAX FX 3 Day WorkoutsДокумент9 страницMAX FX 3 Day WorkoutsJohn SyggelОценок пока нет
- Cast Types and Maintenance InstructionsДокумент32 страницыCast Types and Maintenance InstructionsFerdinand Costales100% (2)
- Manual Muscle Testing: Shoulde R AbductionДокумент14 страницManual Muscle Testing: Shoulde R AbductionDaniJaralОценок пока нет
- Banishing Rituals: The Star RubyДокумент7 страницBanishing Rituals: The Star RubyPieter-Jan BeyulОценок пока нет
- 2 - MMT Elbow FlexorДокумент20 страниц2 - MMT Elbow FlexorDaniJaralОценок пока нет
- Measuring Master For Slopers Document1Документ20 страницMeasuring Master For Slopers Document1nieves21100% (1)
- FCPS SurgeryДокумент97 страницFCPS SurgeryZahid Qamar100% (2)
- Physical Examination of The ElbowДокумент9 страницPhysical Examination of The ElbowpuchioОценок пока нет
- Rotator Cuff and Shoulder Conditioning Program-Orthoinfo - AaosДокумент10 страницRotator Cuff and Shoulder Conditioning Program-Orthoinfo - Aaosapi-228773845100% (1)
- Reading For Comprehension 2 SsДокумент2 страницыReading For Comprehension 2 SsJuan Daniel GilОценок пока нет
- ZhinengqigongggДокумент70 страницZhinengqigongggeeklşeke kelekşlekОценок пока нет
- Board Exam Compilation Book 1 SampleДокумент8 страницBoard Exam Compilation Book 1 Sampleebookwholeseller100% (4)
- Lava Shell Training Manual Hand Arm MassageДокумент2 страницыLava Shell Training Manual Hand Arm MassageAlexandra' LuqueОценок пока нет
- Eldergym e Book 2017Документ106 страницEldergym e Book 2017Anonymous HAaLGGОценок пока нет
- Move Right o-WPS OfficeДокумент2 страницыMove Right o-WPS OfficealjonОценок пока нет
- Flexi Bar Training ManualДокумент27 страницFlexi Bar Training Manualharald0100% (2)
- Anatomy Sem QuestionsДокумент37 страницAnatomy Sem QuestionsRohan sastriОценок пока нет
- Muscles of The Human Body (Origin, Insertion, Innervation, Action)Документ9 страницMuscles of The Human Body (Origin, Insertion, Innervation, Action)Alyssa LumaadОценок пока нет
- 125 - 208 Homework 4 SolutionsДокумент18 страниц125 - 208 Homework 4 SolutionsdfgdfgdfgaaОценок пока нет