Вам также может понравиться
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- An Overview On Tirzepatide, Dual-Targeted Treatment For Diabetes and ObesityДокумент6 страницAn Overview On Tirzepatide, Dual-Targeted Treatment For Diabetes and ObesityInternational Journal of Innovative Science and Research TechnologyОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Psychiatry High Yield NotesДокумент6 страницPsychiatry High Yield Notesgregry2100% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Veterinary Drug Formulary2014 English PDFДокумент19 страницVeterinary Drug Formulary2014 English PDFSamuel LamОценок пока нет
- TICKLER-PRINT Pedia PDFДокумент8 страницTICKLER-PRINT Pedia PDFCarlos H. AcuñaОценок пока нет
- Hyperemesis GravidarumДокумент31 страницаHyperemesis GravidarumDastan HadiОценок пока нет
- Circulation and RespirationДокумент18 страницCirculation and Respirationmursidstone.mursidОценок пока нет
- Recommendations For The Cardiovascular Screening of AthletesДокумент8 страницRecommendations For The Cardiovascular Screening of Athletesmursidstone.mursidОценок пока нет
- EDIT Respiratory Failure Assessment and Problem SolvingДокумент66 страницEDIT Respiratory Failure Assessment and Problem Solvingmursidstone.mursidОценок пока нет
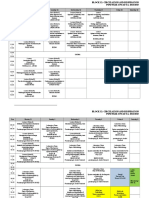
- Revisi Jadwal Blok 12 PK - 2015Документ7 страницRevisi Jadwal Blok 12 PK - 2015mursidstone.mursidОценок пока нет
- Lampiran 2 Analisis Data Pengujian Distribusi Data: Case Processing SummaryДокумент8 страницLampiran 2 Analisis Data Pengujian Distribusi Data: Case Processing Summarymursidstone.mursidОценок пока нет
- Anova Atp Basf Che Adenosine Trifosfat: Analysis of VariansДокумент1 страницаAnova Atp Basf Che Adenosine Trifosfat: Analysis of Variansmursidstone.mursidОценок пока нет
- Daftar Pustaka: Systematic Review. WHO. (Cited 2016 September 03) - Available FromДокумент6 страницDaftar Pustaka: Systematic Review. WHO. (Cited 2016 September 03) - Available Frommursidstone.mursidОценок пока нет
- Aedes Sp. Analysis of Variance Baden Aniline and Soda FactoryДокумент3 страницыAedes Sp. Analysis of Variance Baden Aniline and Soda Factorymursidstone.mursidОценок пока нет
- Balai Litbang P2B2Документ1 страницаBalai Litbang P2B2mursidstone.mursidОценок пока нет
- Analysis of Variance: LC: Lethal Concentration 50 LDДокумент1 страницаAnalysis of Variance: LC: Lethal Concentration 50 LDmursidstone.mursidОценок пока нет
- Daftar Pustak1Документ4 страницыDaftar Pustak1mursidstone.mursidОценок пока нет
- Drug and Therapeutics Committee: Standard Treatment GuidelinesДокумент26 страницDrug and Therapeutics Committee: Standard Treatment Guidelinesmursidstone.mursidОценок пока нет
- Six Steps On Prescribing: Rustamaji/dr. Fian Faculty of Medicine Universitas Gadjah Mada/ Univ Tadulako 2016Документ28 страницSix Steps On Prescribing: Rustamaji/dr. Fian Faculty of Medicine Universitas Gadjah Mada/ Univ Tadulako 2016mursidstone.mursidОценок пока нет
- List of GMP Companies - 2018!03!18Документ2 страницыList of GMP Companies - 2018!03!18Dapper Yourself100% (1)
- Content Owner: Chetan Kothari Compiled By: Abhishek MurarkaДокумент25 страницContent Owner: Chetan Kothari Compiled By: Abhishek MurarkaJ.BОценок пока нет
- PCol - AnesthДокумент6 страницPCol - AnesthRichelle100% (1)
- Chapter Quiz For Antimicrobial AgentsДокумент1 страницаChapter Quiz For Antimicrobial AgentsIrwan M. IskoberОценок пока нет
- Evaluation of Price Disparity Among Generic Medicines in IndiaДокумент3 страницыEvaluation of Price Disparity Among Generic Medicines in Indiadada patilОценок пока нет
- ADC 2023 Landscape Review Part 1 The Drug LandscapeДокумент16 страницADC 2023 Landscape Review Part 1 The Drug LandscapeErick CoОценок пока нет
- Mirabegron StudyДокумент10 страницMirabegron StudyTomás PiccoloОценок пока нет
- Oxytocin Drug StudyДокумент2 страницыOxytocin Drug StudyFernandez, Florence NicoleОценок пока нет
- Industry Analysis The Top 75 Available Cannabis Dispensary Name IdeasДокумент5 страницIndustry Analysis The Top 75 Available Cannabis Dispensary Name IdeasMartin SandersonОценок пока нет
- PHC461 2021 Lab Practical ResultsДокумент3 страницыPHC461 2021 Lab Practical ResultsYuchuk SatuОценок пока нет
- SPC Awarded Tenders Pharmaceutical 2016 OctoberДокумент12 страницSPC Awarded Tenders Pharmaceutical 2016 OctoberKulenthirarajah KobishanthОценок пока нет
- Drug Study InsulinДокумент2 страницыDrug Study InsulinGrant Kenneth Dumo AmigableОценок пока нет
- Pristiq (Desvenlafaxine) Product Monograph For CanadaДокумент48 страницPristiq (Desvenlafaxine) Product Monograph For CanadajennabushОценок пока нет
- Adjuvant Local Anestesi PNBДокумент23 страницыAdjuvant Local Anestesi PNBBangkit PrimayudhaОценок пока нет
- FDA AlertДокумент2 страницыFDA AlertAnonymous Pb39klJОценок пока нет
- Differences in Toxicokinetics and PharmacokineticsДокумент6 страницDifferences in Toxicokinetics and PharmacokineticsnagpharmaaОценок пока нет
- Drugs in Pregnancy: An Update: Journal of SAFOG December 2014Документ6 страницDrugs in Pregnancy: An Update: Journal of SAFOG December 2014BhefHarmoniLoveОценок пока нет
- Steroids in Dentistry: Presented By-Shibani Sarangi Postgraduate Iind Year (Dept of Oral & Maxillofacial Surgery)Документ67 страницSteroids in Dentistry: Presented By-Shibani Sarangi Postgraduate Iind Year (Dept of Oral & Maxillofacial Surgery)Max FaxОценок пока нет
- Module No. 1 Administration of MedicationДокумент7 страницModule No. 1 Administration of Medicationerica nclsОценок пока нет
- 2020 Drug PricesДокумент25 страниц2020 Drug PricesChris-Goldie LorezoОценок пока нет
- Indian Drug Manufacturers: Browse The Diseases AlphabeticallyДокумент4 страницыIndian Drug Manufacturers: Browse The Diseases AlphabeticallyUday kumarОценок пока нет
- Biowaiver ApproachДокумент11 страницBiowaiver Approachmarco hernandezОценок пока нет
- ICT NO. Storage Bin Material Item Description Batch NumberДокумент21 страницаICT NO. Storage Bin Material Item Description Batch NumberInventory MovementОценок пока нет
- Buy Etizolam 3 MG Dosage Tablet Online UKДокумент1 страницаBuy Etizolam 3 MG Dosage Tablet Online UKBuy Zopiclone OnlineОценок пока нет
- G9-Health-2nd-Quarter-Week-1 - 3Документ9 страницG9-Health-2nd-Quarter-Week-1 - 3Catherine Sagario OliquinoОценок пока нет