Вам также может понравиться
- Management of Tuberculosis: A guide for clinicians (eBook edition)От EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Оценок пока нет
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsОт EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsОценок пока нет
- StrokeДокумент74 страницыStrokeDonnaBells Hermo Labaniego100% (2)
- Stroke ManagementДокумент18 страницStroke ManagementAETCM Emergency medicineОценок пока нет
- Hypertension FinalДокумент64 страницыHypertension FinalrameshbmcОценок пока нет
- SyncopeДокумент28 страницSyncopeDurgesh PushkarОценок пока нет
- Congestive Heart FailureДокумент47 страницCongestive Heart FailureRajesh Sharma100% (1)
- SAMДокумент108 страницSAMAlimyon Abilar MontoloОценок пока нет
- Arrhythmia: Presenter-Dr Praveen Kumar Moderator - DR Sandhya ChauhanДокумент71 страницаArrhythmia: Presenter-Dr Praveen Kumar Moderator - DR Sandhya ChauhanDr Praveen100% (1)
- Organo Phosphate Poisoning by DR Gireesh Kumar K PДокумент16 страницOrgano Phosphate Poisoning by DR Gireesh Kumar K PAETCM Emergency medicineОценок пока нет
- Congestive Heart Failure PDFДокумент49 страницCongestive Heart Failure PDFVerinice NañascaОценок пока нет
- Pulmonary EmbolismДокумент80 страницPulmonary EmbolismVarun B Renukappa100% (1)
- Cerebrovascular AccidentДокумент29 страницCerebrovascular AccidentMarites GalvezОценок пока нет
- 02 Bronchial Asthma Circ 2018-2019Документ15 страниц02 Bronchial Asthma Circ 2018-2019Mooha Alanzy100% (1)
- Neuro Vital Signs: Special RotationДокумент6 страницNeuro Vital Signs: Special RotationJamaica LimejuiceОценок пока нет
- HyponatremiaДокумент44 страницыHyponatremiaALi TaLib ShukurОценок пока нет
- Cerebrovascular Accident (CVA)Документ71 страницаCerebrovascular Accident (CVA)nur muizzah afifah hussinОценок пока нет
- Amniotic Fluid EmbolismДокумент29 страницAmniotic Fluid EmbolismArun Kumar Gupta100% (1)
- Evaluation and Management of Suspected Sepsis and Septic by DR Gireesh Kumar K PДокумент36 страницEvaluation and Management of Suspected Sepsis and Septic by DR Gireesh Kumar K PSreekrishnan TrikkurОценок пока нет
- On Emergency DrugsДокумент25 страницOn Emergency DrugsBikram Chhetry100% (1)
- Mood StabilizerДокумент2 страницыMood Stabilizernmyza89Оценок пока нет
- Case Presentation On Ischemic Stroke: G.Hari Prakash Pharm.D InternДокумент22 страницыCase Presentation On Ischemic Stroke: G.Hari Prakash Pharm.D InterngeethaОценок пока нет
- Cardiogenic Shock: Cardiogenic Shock Is Based Upon An Inadequate Circulation ofДокумент5 страницCardiogenic Shock: Cardiogenic Shock Is Based Upon An Inadequate Circulation ofhabeeb23Оценок пока нет
- Chronic Renal FailureДокумент46 страницChronic Renal Failurestepharry08100% (1)
- Antianginal Drugs - Classification and MechanismДокумент1 страницаAntianginal Drugs - Classification and MechanismAhmed YT100% (1)
- Management of Hypertensive Emergency and UrgencyДокумент20 страницManagement of Hypertensive Emergency and UrgencyOersted EdwardОценок пока нет
- AnemiaДокумент47 страницAnemiaAjay KumarОценок пока нет
- Acute Rheumatic Fever - Clinical Manifestations and Diagnosis - UpToDateДокумент15 страницAcute Rheumatic Fever - Clinical Manifestations and Diagnosis - UpToDateDannyGutierrezОценок пока нет
- Case Presentation: Cagayan Valley Medical CenterДокумент57 страницCase Presentation: Cagayan Valley Medical CenterGian PagadduОценок пока нет
- Notes On History Taking in The Cardiovascular SystemДокумент10 страницNotes On History Taking in The Cardiovascular Systemmdjohar72Оценок пока нет
- Cardiovascular DrugsДокумент12 страницCardiovascular DrugshannahcoОценок пока нет
- 9 Ketamine Drug StudyДокумент7 страниц9 Ketamine Drug Studyshadow gonzalezОценок пока нет
- Critical Care Environment - Design Stucture and FacilitiesДокумент22 страницыCritical Care Environment - Design Stucture and FacilitiesProf. Ramsharan MehtaОценок пока нет
- 1 - Fluid and Electrolytes (Schwartz Based)Документ52 страницы1 - Fluid and Electrolytes (Schwartz Based)Alexandra RebosuraОценок пока нет
- Systemic Lupus ErythematosusДокумент37 страницSystemic Lupus ErythematosusFirman Ichlasul AmalОценок пока нет
- LA Myxoma Case PresentationДокумент34 страницыLA Myxoma Case PresentationWiwik Puji LestariОценок пока нет
- Preoperative Assessment in Diabetic PatientsДокумент2 страницыPreoperative Assessment in Diabetic PatientsShilpa Pradhan100% (1)
- SNAKE BITE MEDICAL MANAGEMENT CrebonДокумент33 страницыSNAKE BITE MEDICAL MANAGEMENT Crebonbayu riko100% (1)
- Product Information Avil Product NamesДокумент4 страницыProduct Information Avil Product Namesindyanexpress100% (1)
- Hemorrhagic Cerebro Vascular DiseaseДокумент37 страницHemorrhagic Cerebro Vascular Diseasejbvaldez100% (1)
- 6 Kuliah Liver CirrhosisДокумент55 страниц6 Kuliah Liver CirrhosisAnonymous vUEDx8100% (1)
- Endometriosis O&g PresentationДокумент31 страницаEndometriosis O&g PresentationChauthiran Agamudaiyar100% (1)
- Case Presentation On Scrub TyphusДокумент31 страницаCase Presentation On Scrub TyphusManojОценок пока нет
- AtropineДокумент13 страницAtropineMostafa HassanОценок пока нет
- Acute Myocardial Infarction by DR Gireesh Kumar K PДокумент18 страницAcute Myocardial Infarction by DR Gireesh Kumar K PAETCM Emergency medicine50% (2)
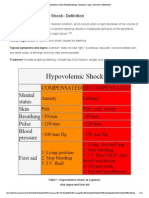
- Hypovolemic Shock Pathophysiology, Symptoms, Signs, Treatment - EHealthStarДокумент15 страницHypovolemic Shock Pathophysiology, Symptoms, Signs, Treatment - EHealthStarKaloy KamaoОценок пока нет
- 3.1.3.2 - HeadacheДокумент40 страниц3.1.3.2 - HeadacheaddinaОценок пока нет
- Renal Cell CarcinomaДокумент1 страницаRenal Cell CarcinomaBobet ReñaОценок пока нет
- Chronic Renal FailureДокумент14 страницChronic Renal FailureyazzzОценок пока нет
- Management of HIV/AIDS by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaДокумент13 страницManagement of HIV/AIDS by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaSreekrishnan TrikkurОценок пока нет
- Infective EndocarditisДокумент68 страницInfective EndocarditisDr. Rajesh PadhiОценок пока нет
- Hypertensive Emergencies: Sulaiman Usaid G. MBCHB V Facilatator: DR Jack TДокумент44 страницыHypertensive Emergencies: Sulaiman Usaid G. MBCHB V Facilatator: DR Jack TUsaid SulaimanОценок пока нет
- Peds Presentation MeningitisДокумент20 страницPeds Presentation Meningitisapi-533578725Оценок пока нет
- Snake Bite ToxiconДокумент14 страницSnake Bite ToxiconAETCM Emergency medicine100% (1)
- DiltiazemДокумент12 страницDiltiazemKalpit SahooОценок пока нет
- Renal CalculiДокумент10 страницRenal CalculiHarpreet Singh100% (1)
- Hepatic Encephalopathy Is by DR Gireesh Kumar K PДокумент16 страницHepatic Encephalopathy Is by DR Gireesh Kumar K PAETCM Emergency medicineОценок пока нет
- Eye Banking: DR - Ajai Agrawal Additional Professor Department of Ophthalmology A.I.I.M.S. RishikeshДокумент56 страницEye Banking: DR - Ajai Agrawal Additional Professor Department of Ophthalmology A.I.I.M.S. RishikeshSrishti KhullarОценок пока нет
- Thyroid Function TestДокумент21 страницаThyroid Function TestPat JacintoОценок пока нет
- AsthmaДокумент23 страницыAsthmaAisyah IcahОценок пока нет
- Stroke 3Документ30 страницStroke 3Aisyah IcahОценок пока нет
- Cognitive Rehab For StrokeДокумент19 страницCognitive Rehab For StrokeAisyah IcahОценок пока нет
- Stroke 1Документ35 страницStroke 1Aisyah IcahОценок пока нет
- A Lion and A MouseДокумент14 страницA Lion and A MouseAisyah IcahОценок пока нет
- Asthma: Name: Aisyah NPM: 12-168Документ23 страницыAsthma: Name: Aisyah NPM: 12-168Aisyah IcahОценок пока нет
- Manual Lifting TechniquesДокумент9 страницManual Lifting Techniquesst_fanucОценок пока нет
- Coaches Checklist For Offensive Game Planning and Goaline Play Calling SeriesДокумент10 страницCoaches Checklist For Offensive Game Planning and Goaline Play Calling Seriesw_dees100% (1)
- VSR 511Документ258 страницVSR 511VenkatapradeepОценок пока нет
- Daniel M. Repola and D.R. Firewood, a Sole Proprietorship, Irene Stevens Repola, His Wife v. Morbark Industries, Inc., a Corporation of the State of Michigan and Morbark Pennsylvania, Inc., a Corporation of the State of Pennsylvania, 934 F.2d 483, 3rd Cir. (1991)Документ22 страницыDaniel M. Repola and D.R. Firewood, a Sole Proprietorship, Irene Stevens Repola, His Wife v. Morbark Industries, Inc., a Corporation of the State of Michigan and Morbark Pennsylvania, Inc., a Corporation of the State of Pennsylvania, 934 F.2d 483, 3rd Cir. (1991)Scribd Government DocsОценок пока нет
- Anatomy Answer KeyДокумент16 страницAnatomy Answer Keylovelots1234Оценок пока нет
- Musculoskeletal MED SURGДокумент57 страницMusculoskeletal MED SURGlolo0880Оценок пока нет
- Assessing The Neurological System: Preparation Mastered CommentsДокумент9 страницAssessing The Neurological System: Preparation Mastered CommentsJo PigarОценок пока нет
- Prestressed Concrete Pipes, Tanks& PolesДокумент36 страницPrestressed Concrete Pipes, Tanks& PolesS PraveenkumarОценок пока нет
- Dynamic Risk Assessment For T & C Activities of 115kV GIS UpdatedДокумент7 страницDynamic Risk Assessment For T & C Activities of 115kV GIS UpdatedwajiОценок пока нет
- Materials and Equipment Request FormДокумент3 страницыMaterials and Equipment Request FormFN5052023 PRAMITA MAHENDRANОценок пока нет
- Orthopedic Exam Notes Apu PDFДокумент6 страницOrthopedic Exam Notes Apu PDFabiramirajalaksmiОценок пока нет
- Human Bones From A Late Minoan IB House at KnossosДокумент74 страницыHuman Bones From A Late Minoan IB House at KnossosAsterios AidonisОценок пока нет
- Link Segment AnalysisДокумент33 страницыLink Segment AnalysisKhaled Abuzayan0% (1)
- Corner Back DrillsДокумент16 страницCorner Back DrillsDrew43stl100% (1)
- Risk Assessment Tower Erection WorkДокумент4 страницыRisk Assessment Tower Erection WorkMuhammad Umar67% (6)
- Vishous Discovers Butch's Secret FantasyДокумент14 страницVishous Discovers Butch's Secret FantasyNatalya Wilson100% (3)
- Dark Elves 2 - Jet Mykles - Mastered ElvesДокумент141 страницаDark Elves 2 - Jet Mykles - Mastered ElvesStLunatic80% (5)
- Biopsychology, 6/E: ISBN: 0-205-42651-4Документ30 страницBiopsychology, 6/E: ISBN: 0-205-42651-4Gînțăgan Denisa GabrielaОценок пока нет
- Neurology Clerkship Study GuideДокумент84 страницыNeurology Clerkship Study GuideShunqing ZhangОценок пока нет
- Monthly Hse Performance Report Related Document: Prime Contractor? Yes NoДокумент3 страницыMonthly Hse Performance Report Related Document: Prime Contractor? Yes NoAKOMOLAFE ABAYOMIОценок пока нет
- CCPG The Use of Enteral Nutrition vs. Parenteral Nutrition PDFДокумент17 страницCCPG The Use of Enteral Nutrition vs. Parenteral Nutrition PDFMario TGОценок пока нет
- Structured Oral Examination in Clinical Anaesthesia Practice Ex NДокумент578 страницStructured Oral Examination in Clinical Anaesthesia Practice Ex Nkaran27091% (11)
- Bauer Reversible Hammer Drill 1992e B ManualДокумент18 страницBauer Reversible Hammer Drill 1992e B ManualBinyamin AcevedoОценок пока нет
- ProcedureeeДокумент160 страницProcedureeeAkhedОценок пока нет
- Three Injured in Crash Near Route 9Документ5 страницThree Injured in Crash Near Route 9Laura Peters ShapiroОценок пока нет
- Hot Topics 4 MonthsДокумент2 страницыHot Topics 4 MonthsPathways AwarenessОценок пока нет
- 2019-06-01 Muscle & FitnessДокумент210 страниц2019-06-01 Muscle & Fitnessjason ivanov100% (1)
- Genital Tract InjuriesДокумент19 страницGenital Tract InjuriesMarvella Nongkhar100% (1)
- Calalas Vs CA, Sunga, SalvaДокумент2 страницыCalalas Vs CA, Sunga, SalvaOlek Dela CruzОценок пока нет