Вам также может понравиться
- Cikini Pengelolaan Nyeri FinalДокумент85 страницCikini Pengelolaan Nyeri FinalisabellaruthhhОценок пока нет
- Case Study of Chronic Hypertension With Superimposed Preeclampsia (Obstetrical Complex)Документ13 страницCase Study of Chronic Hypertension With Superimposed Preeclampsia (Obstetrical Complex)Ivan Laurentine AceretОценок пока нет
- Drug Study Oxytocin and LidocaineДокумент3 страницыDrug Study Oxytocin and LidocaineHazel Grace AhitoОценок пока нет
- PathophysiologyДокумент2 страницыPathophysiologyNERISSA CABRIADASОценок пока нет
- Chest Pain EvaluationДокумент2 страницыChest Pain Evaluatione-MedTools100% (5)
- Mari Zita Spa OnДокумент57 страницMari Zita Spa OnMarty BrownОценок пока нет
- DR Drug Study: 401 2nd SemДокумент2 страницыDR Drug Study: 401 2nd SemHazel Grace AhitoОценок пока нет
- OB Drug Study - OxytocinДокумент3 страницыOB Drug Study - OxytocinJustin AncogОценок пока нет
- Inkontinensia Urin: Dr. Adhi Permana, SPPDДокумент35 страницInkontinensia Urin: Dr. Adhi Permana, SPPDTiara KhairinaОценок пока нет
- Bladder Function and Dysfunction After Neurologic Insult: Preventing Secondary Conditions and Improving FunctionДокумент76 страницBladder Function and Dysfunction After Neurologic Insult: Preventing Secondary Conditions and Improving FunctionakuphysioОценок пока нет
- Sti Mul Atio Nof Uter Ine Cont Assess Vital Signs: Drug Study GuideДокумент8 страницSti Mul Atio Nof Uter Ine Cont Assess Vital Signs: Drug Study GuideAubrey SungaОценок пока нет
- Mini Case Study 1Документ14 страницMini Case Study 1Casas, Jo-an Pauline A.Оценок пока нет
- CASE STUDY PheumoniaДокумент5 страницCASE STUDY PheumoniaEdelweiss Marie CayetanoОценок пока нет
- MethergineДокумент2 страницыMethergineKyla VillafrancaОценок пока нет
- Drug Study LeukemiaДокумент12 страницDrug Study LeukemiaLiana CervantesОценок пока нет
- Lesson Plan Hisschsprung DiseaseДокумент10 страницLesson Plan Hisschsprung DiseasePPG Selvi Jebakani IsaacОценок пока нет
- PALS (Pediatric Advanced Life Support)Документ48 страницPALS (Pediatric Advanced Life Support)Jackson HakimОценок пока нет
- Drug Study TL.Документ19 страницDrug Study TL.Maria Teresa VillanuevaОценок пока нет
- Congenital Adrenal HyperplasiaДокумент28 страницCongenital Adrenal HyperplasiaWindelyn Gamaro0% (1)
- Chapter 32 Cholinergic AgonistsДокумент2 страницыChapter 32 Cholinergic AgonistsJaira EmmarinaОценок пока нет
- Acute Flaccid ParalysisДокумент34 страницыAcute Flaccid ParalysisMentari Alisha100% (1)
- Biosynthesis and Physiologic Effects of Estrogen and Pathophysiologic Effects of Estrogen Deficiency: A ReviewДокумент4 страницыBiosynthesis and Physiologic Effects of Estrogen and Pathophysiologic Effects of Estrogen Deficiency: A Reviewsurya antoОценок пока нет
- CITICOLINE, Drugs in MedicalДокумент10 страницCITICOLINE, Drugs in MedicalInosanto May AnnОценок пока нет
- (GYNE) Dysmenorrhea and Breast Diseases-Dr. Lim (Pingu)Документ13 страниц(GYNE) Dysmenorrhea and Breast Diseases-Dr. Lim (Pingu)adrian kristopher dela cruzОценок пока нет
- Drug StudyДокумент15 страницDrug Studyjustine franchesca abonОценок пока нет
- Evangelista Drug-StudyДокумент15 страницEvangelista Drug-Studydinglasanerica57Оценок пока нет
- PATH All TA Reviews Answers and Notes11Документ718 страницPATH All TA Reviews Answers and Notes11Andleeb Imran100% (1)
- Drug Name Action Indication Contraindication Side Effects Nsg. ConsiderationДокумент6 страницDrug Name Action Indication Contraindication Side Effects Nsg. ConsiderationjeremyescaraОценок пока нет
- Predisposing Factor Modifiable Precipitating FactorДокумент6 страницPredisposing Factor Modifiable Precipitating FactorAicir TapОценок пока нет
- Pathways Colitis Cerative Group 1Документ3 страницыPathways Colitis Cerative Group 1Fuzna DahliaОценок пока нет
- Urinary Incontinence in The Aging Patient: DR Putra Hendra SPPD UnibaДокумент34 страницыUrinary Incontinence in The Aging Patient: DR Putra Hendra SPPD UnibaRetno Tri HaryatiОценок пока нет
- Asfixia Perinatal, CompendiumДокумент7 страницAsfixia Perinatal, CompendiumClaudia LópezОценок пока нет
- Drug Study: I Loilo Doctors' College College of NursingДокумент6 страницDrug Study: I Loilo Doctors' College College of NursingAudrie Allyson GabalesОценок пока нет
- 2012 The Patient History - Evidence Based Appoach-368-376 PDFДокумент9 страниц2012 The Patient History - Evidence Based Appoach-368-376 PDFJoseph AndradeОценок пока нет
- Clinical Analysis: I. Patient's ProfileДокумент19 страницClinical Analysis: I. Patient's ProfileKathleen DimacaliОценок пока нет
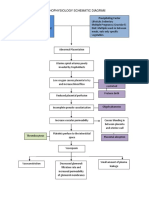
- Pathophysiology Schematic Diagram: Predisposing Factor Precipitating FactorДокумент4 страницыPathophysiology Schematic Diagram: Predisposing Factor Precipitating FactorCarrie A100% (2)
- Case Study Preeclampsia FinДокумент5 страницCase Study Preeclampsia FinAngel Clarisse JariolОценок пока нет
- Drug Study HerniaДокумент4 страницыDrug Study HerniawendyОценок пока нет
- Ds in Delivery RoomДокумент11 страницDs in Delivery RoomArian May MarcosОценок пока нет
- 13 March 2015 Dr. Eimear Fagan Eimear - Fagan@ncl - Ac.ukДокумент33 страницы13 March 2015 Dr. Eimear Fagan Eimear - Fagan@ncl - Ac.ukshirley_ling_15Оценок пока нет
- Oxytocin: Drug ChartДокумент2 страницыOxytocin: Drug Chartklirt carayoОценок пока нет
- Inkontinensia Urin: Dr. Adhi Permana, SPPDДокумент35 страницInkontinensia Urin: Dr. Adhi Permana, SPPDtutor tujuhОценок пока нет
- ER Drug StudyДокумент4 страницыER Drug StudyNecy Tessa C. AcostaОценок пока нет
- Pancreatitis Group 3 NCM 116Документ21 страницаPancreatitis Group 3 NCM 116Diana Jane LauretaОценок пока нет
- Preterm Labor, Hyperemesis Gravidarum - PathophysiologyДокумент2 страницыPreterm Labor, Hyperemesis Gravidarum - PathophysiologyreyneldanОценок пока нет
- Paracetamol Tramadol KCLДокумент5 страницParacetamol Tramadol KCLDani DaniОценок пока нет
- A Child With An Epileptic Status With Growth FalteringДокумент25 страницA Child With An Epileptic Status With Growth FalteringHasan HusienОценок пока нет
- Benign Prostatic HyperplasiaДокумент5 страницBenign Prostatic Hyperplasiatabangin_hilario100% (1)
- Pathophysiology - UtiДокумент2 страницыPathophysiology - UtiAyessa Marie BarbosaОценок пока нет
- TNCC Study GuideДокумент6 страницTNCC Study Guidekristinekat96% (24)
- What Is TriagingДокумент5 страницWhat Is TriagingshairaОценок пока нет
- PrioritizingДокумент1 страницаPrioritizingSuperNurseОценок пока нет
- Cerebral Aneurysm-Parkinsons DiseaseДокумент3 страницыCerebral Aneurysm-Parkinsons Diseaseanime listОценок пока нет
- LocalДокумент5 страницLocalybqbjpvtmrОценок пока нет
- Approach To Urinary IncontinenceДокумент71 страницаApproach To Urinary IncontinenceArup KhanОценок пока нет
- IntussusceptionДокумент13 страницIntussusceptionwydiake3Оценок пока нет
- Menopause Transition (Klimakterium) : Rila Rindi Antina, S.ST., M.AP., M.KesДокумент18 страницMenopause Transition (Klimakterium) : Rila Rindi Antina, S.ST., M.AP., M.KesMuhas SanahОценок пока нет
- Female Arousal and Orgasm: Anatomy, Physiology, Behaviour and EvolutionОт EverandFemale Arousal and Orgasm: Anatomy, Physiology, Behaviour and EvolutionОценок пока нет
- The Comprehensive Evaluation and Treatment of Epilepsy: A Practical GuideОт EverandThe Comprehensive Evaluation and Treatment of Epilepsy: A Practical GuideОценок пока нет
- Conquering Incontinence: A New and Physical Approach to a Freer LifestyleОт EverandConquering Incontinence: A New and Physical Approach to a Freer LifestyleОценок пока нет
- Dr. Nur Asni-Uterine SubinvolusionДокумент30 страницDr. Nur Asni-Uterine SubinvolusionYhaya 'Dzulhijjahyanti'75% (4)
- Dystocia: Bagian / UP Obgin FK - UNHAS /RS - Dr.Wahidin Sudirohusodo MakassarДокумент69 страницDystocia: Bagian / UP Obgin FK - UNHAS /RS - Dr.Wahidin Sudirohusodo MakassarYhaya 'Dzulhijjahyanti'Оценок пока нет
- Modul 4 Urin Incontinence: Group 14 Problem Base Learning Medical Faculty Muslim University of IndonesiaДокумент22 страницыModul 4 Urin Incontinence: Group 14 Problem Base Learning Medical Faculty Muslim University of IndonesiaYhaya 'Dzulhijjahyanti'Оценок пока нет
- ABC TraumaДокумент5 страницABC TraumaYhaya 'Dzulhijjahyanti'Оценок пока нет
- Primary Survey Secondary Survey: Control/ Go Home If The Condition Is Stable HospitalizeДокумент1 страницаPrimary Survey Secondary Survey: Control/ Go Home If The Condition Is Stable HospitalizeYhaya 'Dzulhijjahyanti'Оценок пока нет
- Ornac Standards PositioningДокумент7 страницOrnac Standards PositioningAndika X NandaОценок пока нет
- (IM Ward) History Taking Tool PDFДокумент15 страниц(IM Ward) History Taking Tool PDFleapacis100% (1)
- Exercise On Strength: Joshua Lester J. ArellanoДокумент17 страницExercise On Strength: Joshua Lester J. ArellanoBryantОценок пока нет
- Calipers - Lower ExtremityДокумент40 страницCalipers - Lower ExtremityNivetha RavikumarОценок пока нет
- Thyroid FunctionДокумент2 страницыThyroid FunctionVishnuga MohanОценок пока нет
- EXCERSIEДокумент6 страницEXCERSIEJessy NairОценок пока нет
- Step 1: Reverse Out Knee PainДокумент11 страницStep 1: Reverse Out Knee PainGrant Cherry100% (3)
- Locking The GateДокумент8 страницLocking The GateShadow_Warrior88100% (1)
- Triceps - 6 KomДокумент3 страницыTriceps - 6 KomMatijaОценок пока нет
- The YMCA Bench Press Test.10Документ4 страницыThe YMCA Bench Press Test.10katerinaОценок пока нет
- Treatment of An Ankylosed Central Incisor by Single Tooth Dento-Osseous Osteotomy and A Simple Distraction DeviceДокумент9 страницTreatment of An Ankylosed Central Incisor by Single Tooth Dento-Osseous Osteotomy and A Simple Distraction DeviceJuan Carlos MeloОценок пока нет
- Yeny Elfiyanti - 1910070100082 - Tugas Praktikum Anatomi 2Документ5 страницYeny Elfiyanti - 1910070100082 - Tugas Praktikum Anatomi 2Yeny ElfiyantiОценок пока нет
- Case Presentation and Literature Review of Adrenal MassesДокумент50 страницCase Presentation and Literature Review of Adrenal MassesAnas Mk HindawiОценок пока нет
- Shoulder Case Study 2Документ5 страницShoulder Case Study 2superhoofy7186Оценок пока нет
- Hipo HiperthyroidДокумент49 страницHipo HiperthyroidMuhammad Bilal Bin AmirОценок пока нет
- Science10 Q3 SLM1 1Документ15 страницScience10 Q3 SLM1 1Bien Divinaflor100% (1)
- DEPARTMENT OF Dental Anatomy, Embryology and Oral Histology: Dr. Diana Prem VMSDC, SalemДокумент25 страницDEPARTMENT OF Dental Anatomy, Embryology and Oral Histology: Dr. Diana Prem VMSDC, SalemDR. H. DIANA J.HENRY CHRISTOPHERОценок пока нет
- Receptor Endings: Dr. Mehwish KhalidДокумент32 страницыReceptor Endings: Dr. Mehwish KhalidSamia AsgharОценок пока нет
- Anatomy & Physiology Unit 1Документ29 страницAnatomy & Physiology Unit 1Priyanjali SainiОценок пока нет
- Anatomy of The Psoas MuscleДокумент2 страницыAnatomy of The Psoas MuscleMilos KovacevicОценок пока нет
- Wa0006Документ30 страницWa0006rushaliОценок пока нет
- Radical Neck Dissection: (RND) Classification, Indication and TechniquesДокумент42 страницыRadical Neck Dissection: (RND) Classification, Indication and TechniquesPatrycyaОценок пока нет
- Topic 2.1 Ventilatory System Sport Science IBДокумент4 страницыTopic 2.1 Ventilatory System Sport Science IBAntonio MouОценок пока нет
- Zanki Neuro BoldedДокумент25 страницZanki Neuro Boldedsmian08Оценок пока нет
- Traumatic Tympanic Membrane PerforationДокумент7 страницTraumatic Tympanic Membrane PerforationNada ZultiОценок пока нет
- CTCB in Mandibular ParesthesiaДокумент3 страницыCTCB in Mandibular ParesthesiaAdrian OlveraОценок пока нет
- Carcinoma BreastДокумент47 страницCarcinoma BreastMayank YadavОценок пока нет
- Animal Physiology: Review For Licensure Exam in AgricultureДокумент152 страницыAnimal Physiology: Review For Licensure Exam in AgricultureJayson BasiagОценок пока нет
- Neuroanatomy An Illustrated Colour Text Crossman 6 Ed 2020 PDFДокумент185 страницNeuroanatomy An Illustrated Colour Text Crossman 6 Ed 2020 PDFKatrin CoolChe100% (3)
- Locate The Image of in A Curved Mirror. Write Your Answer in The TableДокумент7 страницLocate The Image of in A Curved Mirror. Write Your Answer in The TablejowieОценок пока нет