Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- MODULE4 Philosophical and Socio - Anthropological Foundation of Physical Education and SportsДокумент15 страницMODULE4 Philosophical and Socio - Anthropological Foundation of Physical Education and SportsZedy Gulles100% (15)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- F&B Waste Management QuestionnaireДокумент3 страницыF&B Waste Management QuestionnairePranav Kakà Harmilapi70% (27)
- CPSM BasicsДокумент15 страницCPSM BasicsProsenjit Das0% (1)
- UNICEF WASH Officer Job ProfileДокумент5 страницUNICEF WASH Officer Job ProfileazizrbgОценок пока нет
- Tootise Pop LabДокумент3 страницыTootise Pop Labapi-282362086Оценок пока нет
- EVANGELISTA - Assignment #2Документ4 страницыEVANGELISTA - Assignment #2Gabrielle EvangelistaОценок пока нет
- Ule 2015Документ22 страницыUle 2015jhgfjgvjbhОценок пока нет
- Adaptive Reuse As A StrategyДокумент10 страницAdaptive Reuse As A StrategyAlexandru ȚîrcăОценок пока нет
- IIM Nagpur GMP - BrochureДокумент17 страницIIM Nagpur GMP - Brochuregprakash00820Оценок пока нет
- Sucrose Gradient Separation ProtocolДокумент16 страницSucrose Gradient Separation ProtocolBalaОценок пока нет
- Language of Research PG XWD AnsДокумент1 страницаLanguage of Research PG XWD AnsLourhenz AliyacyacОценок пока нет
- Call For Applicants GuidanceДокумент21 страницаCall For Applicants GuidanceMohamedОценок пока нет
- Violence Exposure Among Children With DisabilitiesДокумент21 страницаViolence Exposure Among Children With DisabilitiesPawaniGuptaОценок пока нет
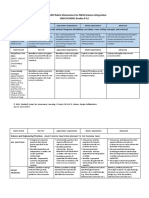
- Ngss Science Integration LDC 9-12 Rubric-3Документ6 страницNgss Science Integration LDC 9-12 Rubric-3api-318937942Оценок пока нет
- Training Module Development For The Health Promotion of Older Persons in The PhilippinesДокумент37 страницTraining Module Development For The Health Promotion of Older Persons in The PhilippinesSherwin PazzibuganОценок пока нет
- The Up To 21-Year Clinical Outcome and Survival of Feldspathic Porcelain Veneers: Accounting For ClusteringДокумент9 страницThe Up To 21-Year Clinical Outcome and Survival of Feldspathic Porcelain Veneers: Accounting For ClusteringAlexander L. Contreras PairaОценок пока нет
- Understanding Comparative Politics PDFДокумент20 страницUnderstanding Comparative Politics PDFHansh Raj HanshuОценок пока нет
- Activity For Central TendencyДокумент3 страницыActivity For Central TendencyJessel TagalogОценок пока нет
- MonographДокумент8 страницMonographtaha shabanОценок пока нет
- Module 1 - Search Engine BasicsДокумент79 страницModule 1 - Search Engine BasicsPRIYANKA TARACHANDANIОценок пока нет
- M.E. Qem FT & PTДокумент63 страницыM.E. Qem FT & PTramasamy rОценок пока нет
- Fluidity in Project Management Teams Across Projects: An Executive SummaryДокумент15 страницFluidity in Project Management Teams Across Projects: An Executive Summarytukang komenОценок пока нет
- Conan Dissertation 2018Документ248 страницConan Dissertation 2018john carlo bengalaОценок пока нет
- Risk Assessment Considerations For Installation of A New AutoclaveДокумент29 страницRisk Assessment Considerations For Installation of A New AutoclaveDoan Chi ThienОценок пока нет
- Esci ResultsДокумент23 страницыEsci Resultsapi-304738945Оценок пока нет
- Syllabus: Maharashtra University of Health Sciences, NashikДокумент5 страницSyllabus: Maharashtra University of Health Sciences, NashikRuchi HumaneОценок пока нет
- Research ArticleДокумент7 страницResearch ArticleleticiaОценок пока нет
- TeachStarter 709102 TeachStarter Starter Sheet Chance and Data Maths Investigation Roll Me A SixДокумент2 страницыTeachStarter 709102 TeachStarter Starter Sheet Chance and Data Maths Investigation Roll Me A SixIuliana IgnatОценок пока нет
- OM-Lecture 2 (Heritage & Productivity)Документ22 страницыOM-Lecture 2 (Heritage & Productivity)Ismatullah ButtОценок пока нет
- Republic of The Philippines Cavitestateuniversity Don Severino Delas Alas Campus Indang, CaviteДокумент1 страницаRepublic of The Philippines Cavitestateuniversity Don Severino Delas Alas Campus Indang, CaviteteuuuuОценок пока нет