Вам также может понравиться
- Use of Rhythmic Wire System With Miniscrews To Correct Occlusal Plane CantingДокумент8 страницUse of Rhythmic Wire System With Miniscrews To Correct Occlusal Plane CantingMaria VeronicaОценок пока нет
- Early Treatment of Vertical Skeletal DysplasiaДокумент11 страницEarly Treatment of Vertical Skeletal Dysplasiagilberto69Оценок пока нет
- Gummy Smile Case ReportДокумент13 страницGummy Smile Case ReportAli ChaconОценок пока нет
- Gummy Smile - IntegrativeДокумент3 страницыGummy Smile - IntegrativeNingombam Robinson SinghОценок пока нет
- Introducing The Wireframe DNA Appliance Singh Lipka JAAGO 2009 ArticleДокумент4 страницыIntroducing The Wireframe DNA Appliance Singh Lipka JAAGO 2009 ArticleAnders CroccoОценок пока нет
- Open bite treatment using posterior tooth intrusionДокумент56 страницOpen bite treatment using posterior tooth intrusionKuang-Wei ShuОценок пока нет
- Variable Torque BracketsДокумент13 страницVariable Torque BracketsnadiaОценок пока нет
- Fixed Orthodontic Appliances: A Practical GuideОт EverandFixed Orthodontic Appliances: A Practical GuideРейтинг: 1 из 5 звезд1/5 (1)
- Article Anterior Open BiteДокумент6 страницArticle Anterior Open BiteDrRudra Chakraborty100% (1)
- Spear-Approaches To Vertical DimensionДокумент11 страницSpear-Approaches To Vertical DimensionMario Zúñiga Gonzales100% (2)
- New Table To Guide Bracket PlacementДокумент4 страницыNew Table To Guide Bracket PlacementDr. Tomas Castellanos100% (2)
- Sterilization in OrthodonticsДокумент121 страницаSterilization in OrthodonticsSwati PawarОценок пока нет
- IndicationДокумент70 страницIndicationPKS 1988Оценок пока нет
- Management of Vertical Maxillary ExcessДокумент24 страницыManagement of Vertical Maxillary ExcesssweetieОценок пока нет
- Development of Dental OcclusionДокумент89 страницDevelopment of Dental OcclusionMothi KrishnaОценок пока нет
- Role of Mini-Implants in OrthodonticsДокумент9 страницRole of Mini-Implants in OrthodonticsRonald WilfredОценок пока нет
- Jiang T 2019Документ9 страницJiang T 2019CLAUDIA PATRICIA ROSALES BASANTEОценок пока нет
- Temporary Anchorage Devices in Orthodontics: A Paradigm ShiftДокумент7 страницTemporary Anchorage Devices in Orthodontics: A Paradigm ShiftsmritiОценок пока нет
- Chaconas NotesДокумент12 страницChaconas NotesOusama DamlajОценок пока нет
- Homeobox GeneДокумент9 страницHomeobox GenesuchitraОценок пока нет
- Twinblockshilpa 170129085958 PDFДокумент130 страницTwinblockshilpa 170129085958 PDFWaqar JeelaniОценок пока нет
- Biology of Tooth Movement - Semair 5Документ138 страницBiology of Tooth Movement - Semair 5Manjunath BellaryОценок пока нет
- Normal Occlusion 1 / Orthodontic Courses by Indian Dental AcademyДокумент20 страницNormal Occlusion 1 / Orthodontic Courses by Indian Dental Academyindian dental academyОценок пока нет
- Cone-Beam Computer TomographyДокумент79 страницCone-Beam Computer Tomographyjohn suryavardhan100% (1)
- Versatile 2x4 Appliance Corrects Crossbites and Aligns TeethДокумент4 страницыVersatile 2x4 Appliance Corrects Crossbites and Aligns Teethvefiisphepy83312Оценок пока нет
- Twin Block Aplliane - Mwangi MuchiriДокумент5 страницTwin Block Aplliane - Mwangi MuchiriAlex M MwangiОценок пока нет
- Multi-Distalizing Arch™ ApplianceДокумент4 страницыMulti-Distalizing Arch™ ApplianceOrtho OrganizersОценок пока нет
- Cone Beam Tomography in Orthodontics PDFДокумент8 страницCone Beam Tomography in Orthodontics PDFdruzair007Оценок пока нет
- Mini Implants in Orthodontics: Review ArticleДокумент5 страницMini Implants in Orthodontics: Review Articledrzana78Оценок пока нет
- Removable Orthodontic Appliances ANALHAQ Class For 3rd Year BDSДокумент72 страницыRemovable Orthodontic Appliances ANALHAQ Class For 3rd Year BDSAnalhaq ShaikhОценок пока нет
- 2 Pioneers and Milestones in The Field of Orthodontics and Orthognathic Surgery 2014 Orthognathic SurgeryДокумент43 страницы2 Pioneers and Milestones in The Field of Orthodontics and Orthognathic Surgery 2014 Orthognathic SurgeryiweourvgiuОценок пока нет
- Diagnostic Imaginf of TMJ - A ReviewДокумент4 страницыDiagnostic Imaginf of TMJ - A ReviewRhea RejiОценок пока нет
- JO Cousley2015-Controlled Canine Retraction Using Orthodontic Mini-Implants Coupled With Bondable Powerarms PDFДокумент9 страницJO Cousley2015-Controlled Canine Retraction Using Orthodontic Mini-Implants Coupled With Bondable Powerarms PDFdrgeorgejose7818Оценок пока нет
- Biomechanics and Tooth Movement in Orthodontics: Ita Purnama Alwi JO55201001 Ppdgs Ortodonti FKG Unhas 2021Документ40 страницBiomechanics and Tooth Movement in Orthodontics: Ita Purnama Alwi JO55201001 Ppdgs Ortodonti FKG Unhas 2021Ortodonti UnhasОценок пока нет
- Review Article: Barry H. Grayson, Pradip R. ShetyeДокумент7 страницReview Article: Barry H. Grayson, Pradip R. ShetyeHARITHA H.PОценок пока нет
- Finishing Orthodontic Treatment for Optimal Esthetics, Function and StabilityДокумент13 страницFinishing Orthodontic Treatment for Optimal Esthetics, Function and StabilityMargarita Lopez Martinez100% (1)
- Neural Crest Cell / Orthodontic Courses by Indian Dental AcademyДокумент108 страницNeural Crest Cell / Orthodontic Courses by Indian Dental Academyindian dental academy100% (1)
- Chris Chang Article PDFДокумент18 страницChris Chang Article PDFTxemi GonzalezОценок пока нет
- Placing TADsДокумент3 страницыPlacing TADsvijayprabugОценок пока нет
- Canine Impaction-A Review of The Prevalence, Etiology, Diagnosis and TreatmentДокумент26 страницCanine Impaction-A Review of The Prevalence, Etiology, Diagnosis and TreatmentAnil MarnaОценок пока нет
- Understanding the History and Mechanisms of the Activator ApplianceДокумент91 страницаUnderstanding the History and Mechanisms of the Activator ApplianceCarlosAndresPabonCortesОценок пока нет
- Badel Michigan Splint and Treatment PDFДокумент9 страницBadel Michigan Splint and Treatment PDF謎超人Оценок пока нет
- Proximal Stripping PDFДокумент11 страницProximal Stripping PDFsmilecarekkmОценок пока нет
- Smile Analysis: A Review Part IIДокумент4 страницыSmile Analysis: A Review Part IIGustavoAndresGarciaОценок пока нет
- The Occlusal Splint TherapyДокумент5 страницThe Occlusal Splint TherapyVíctor Adolfo Ravelo SalinasОценок пока нет
- Vertical Skeletal DysplasiaДокумент119 страницVertical Skeletal DysplasiaAshish Mathew0% (1)
- Skeletal Anchorage Systems in Orthodontics Absolute Anchorage Adream or RealityДокумент10 страницSkeletal Anchorage Systems in Orthodontics Absolute Anchorage Adream or RealitySoe San KyawОценок пока нет
- Bite TurboДокумент6 страницBite TurboOmar DS100% (1)
- Deepbite Correction With Incisor Intrusion inДокумент6 страницDeepbite Correction With Incisor Intrusion inAbad SalcedoОценок пока нет
- Myofunctional AppliancesДокумент179 страницMyofunctional AppliancesSwati PawarОценок пока нет
- TADSДокумент8 страницTADSDIANA PAOLA FONTECHA GONZÁLEZОценок пока нет
- Growth PredictionДокумент64 страницыGrowth PredictionMothi KrishnaОценок пока нет
- Current Topics and Controversies Presented by DR Anthony GianellyДокумент2 страницыCurrent Topics and Controversies Presented by DR Anthony GianellyIvanna H. A.Оценок пока нет
- Activator HeadgearДокумент9 страницActivator HeadgearThendral DevanathanОценок пока нет
- Space AnalysisДокумент8 страницSpace AnalysisMohammed JaberОценок пока нет
- Presurgical Infant Orthopedics For Cleft Lip and PДокумент6 страницPresurgical Infant Orthopedics For Cleft Lip and PPark JiminОценок пока нет
- Tads 1Документ6 страницTads 1travolta0Оценок пока нет
- Twin Block Appliance Guide for Class II and III Malocclusion CorrectionДокумент52 страницыTwin Block Appliance Guide for Class II and III Malocclusion CorrectionAnupamaОценок пока нет
- Bite RegistratnДокумент68 страницBite RegistratnBimalKrishnaОценок пока нет
- Twin Block 01-02-23Документ53 страницыTwin Block 01-02-23AnupamaОценок пока нет
- M.A. Degree Examination, 2010: (Philosophy, Religion and Culture) (First Year) (Paper-Iii) 530. Social EthicsДокумент1 страницаM.A. Degree Examination, 2010: (Philosophy, Religion and Culture) (First Year) (Paper-Iii) 530. Social EthicsBimalKrishnaОценок пока нет
- M.A. Degree Examination, 2011Документ1 страницаM.A. Degree Examination, 2011BimalKrishnaОценок пока нет
- Modern Indian Philosophy Exam QuestionsДокумент1 страницаModern Indian Philosophy Exam QuestionsBimalKrishnaОценок пока нет
- M.A. Degree Examination, 2010: (Philosophy, Religion and Culture) (First Year) (PAPER-V) 550. Temple ManagementДокумент1 страницаM.A. Degree Examination, 2010: (Philosophy, Religion and Culture) (First Year) (PAPER-V) 550. Temple ManagementBimalKrishnaОценок пока нет
- M.A. Degree Examination, 2011: 520. Comparative ReligionДокумент2 страницыM.A. Degree Examination, 2011: 520. Comparative ReligionBimalKrishnaОценок пока нет
- M.A. Degree Examination, 2011: 610. Modern Indian PhilosophyДокумент2 страницыM.A. Degree Examination, 2011: 610. Modern Indian PhilosophyBimalKrishnaОценок пока нет
- M.A. Degree Examination, 2011: 650. SaivismДокумент2 страницыM.A. Degree Examination, 2011: 650. SaivismBimalKrishnaОценок пока нет
- M.A. Degree Examination, 2010: (Philosophy, Religion and Culture) (First Year) (Paper-Ii) 520. Comparative ReligionДокумент1 страницаM.A. Degree Examination, 2010: (Philosophy, Religion and Culture) (First Year) (Paper-Ii) 520. Comparative ReligionBimalKrishnaОценок пока нет
- Indian Philosophy Exam QuestionsДокумент1 страницаIndian Philosophy Exam QuestionsBimalKrishnaОценок пока нет
- M.A. Degree Examination, 2011: 540. Indian Culture - IДокумент2 страницыM.A. Degree Examination, 2011: 540. Indian Culture - IBimalKrishnaОценок пока нет
- M.A. Degree Examination, 2011: 640. Indian Culture - IiДокумент2 страницыM.A. Degree Examination, 2011: 640. Indian Culture - IiBimalKrishnaОценок пока нет
- M.A. Degree Examination - 2012: Total No. of Pages: 1Документ1 страницаM.A. Degree Examination - 2012: Total No. of Pages: 1BimalKrishnaОценок пока нет
- M.A. Degree Examination, 2011: 630. Logic and Scientific MethodsДокумент2 страницыM.A. Degree Examination, 2011: 630. Logic and Scientific MethodsBimalKrishnaОценок пока нет
- M.A. Degree Examination, 2011: 620. Western PhilosophyДокумент2 страницыM.A. Degree Examination, 2011: 620. Western PhilosophykmbkrisОценок пока нет
- M.A. Degree Examination, 2011Документ1 страницаM.A. Degree Examination, 2011BimalKrishnaОценок пока нет
- M.A. Degree Examination, 2011: 530. Social EthicsДокумент2 страницыM.A. Degree Examination, 2011: 530. Social EthicsNirmala1987Оценок пока нет
- Saiva Siddhanta Diploma Exam PapersДокумент43 страницыSaiva Siddhanta Diploma Exam PapersBimalKrishnaОценок пока нет
- M.A. Degree Examination, 2011: 520. Comparative ReligionДокумент2 страницыM.A. Degree Examination, 2011: 520. Comparative ReligionBimalKrishnaОценок пока нет
- New Doc 2019-10-22 17.34.52 PDFДокумент1 страницаNew Doc 2019-10-22 17.34.52 PDFBimalKrishnaОценок пока нет
- UcchishtaganesaДокумент8 страницUcchishtaganesaBimalKrishnaОценок пока нет
- M.A. Degree Examination - 2013: Total No. of Pages: 1Документ1 страницаM.A. Degree Examination - 2013: Total No. of Pages: 1BimalKrishnaОценок пока нет
- M.A. Degree Examination, 2010: (Philosophy, Religion and Culture) (First Year) (Paper-Ii) 520. Comparative ReligionДокумент1 страницаM.A. Degree Examination, 2010: (Philosophy, Religion and Culture) (First Year) (Paper-Ii) 520. Comparative ReligionBimalKrishnaОценок пока нет
- Diploma Examination - 2011: (Saiva Siddhanta)Документ3 страницыDiploma Examination - 2011: (Saiva Siddhanta)BimalKrishnaОценок пока нет
- AppraisalДокумент6 страницAppraisaldhar_sohini6225Оценок пока нет
- M.A. Degree Examination - 2012: Total No. of Pages: 1Документ1 страницаM.A. Degree Examination - 2012: Total No. of Pages: 1BimalKrishnaОценок пока нет
- AppraisalДокумент6 страницAppraisaldhar_sohini6225Оценок пока нет
- M.A. Degree Examination - 2012: Total No. of Pages: 1Документ1 страницаM.A. Degree Examination - 2012: Total No. of Pages: 1BimalKrishnaОценок пока нет
- M.A. Degree Examination, 2011Документ1 страницаM.A. Degree Examination, 2011BimalKrishnaОценок пока нет
- M.A. Degree Examination - 2012: Total No. of Pages: 1Документ1 страницаM.A. Degree Examination - 2012: Total No. of Pages: 1BimalKrishnaОценок пока нет
- M.A. Degree Examination, 2011: 630. Logic and Scientific MethodsДокумент2 страницыM.A. Degree Examination, 2011: 630. Logic and Scientific MethodsBimalKrishnaОценок пока нет
- Section I #18 The Temporomandibular JointДокумент3 страницыSection I #18 The Temporomandibular JointInnocent L NdambakuwaОценок пока нет
- Chinese-Medical Terminology 33023 PDFДокумент1 страницаChinese-Medical Terminology 33023 PDFYS NateОценок пока нет
- Physical Fitness GuideДокумент9 страницPhysical Fitness GuidePaulyn Jhoy FajardoОценок пока нет
- The Muscular System: AIM: To Understand The Structure and Function of MusclesДокумент28 страницThe Muscular System: AIM: To Understand The Structure and Function of MusclespuhiОценок пока нет
- Enteric Nervous SystemДокумент5 страницEnteric Nervous Systemmehdi mafakheriОценок пока нет
- Anatomy and Physiology I (BIO201) Course MaterialsДокумент18 страницAnatomy and Physiology I (BIO201) Course MaterialsAnnie Minnie0% (1)
- Jurnal Unilateral Cleft LipДокумент11 страницJurnal Unilateral Cleft LipTriasnidaОценок пока нет
- Penegakan Diagnosis Dan Penanggulangan Cervicalys Herniated: Nucleus PulposusДокумент12 страницPenegakan Diagnosis Dan Penanggulangan Cervicalys Herniated: Nucleus PulposusMuhammad Rizki Mardiansyah MardiansyahОценок пока нет
- Boundless Anatomy and Physiology: Overview of the Urinary SystemДокумент3 страницыBoundless Anatomy and Physiology: Overview of the Urinary Systemor1da2sa3Оценок пока нет
- Comparative anatomy of vertebrate urogenital systemsДокумент3 страницыComparative anatomy of vertebrate urogenital systems999s jamОценок пока нет
- 1advances in Occlusion Anterior GuidanceДокумент29 страниц1advances in Occlusion Anterior GuidanceSalem RawashdahОценок пока нет
- CH 15Документ26 страницCH 15Mohd Khairidzman BoeranОценок пока нет
- PAR Q & YOU: ASSESS YOUR FITNESS LEVELДокумент9 страницPAR Q & YOU: ASSESS YOUR FITNESS LEVELMark BermejoОценок пока нет
- Science Q3 Nerv - SystemДокумент4 страницыScience Q3 Nerv - SystemSophia AnamaОценок пока нет
- Tips and Tools To Vocal FreedomДокумент10 страницTips and Tools To Vocal FreedomasifОценок пока нет
- Rudraksha For Rashi and NakshatrasДокумент2 страницыRudraksha For Rashi and NakshatrasDeepak SethiОценок пока нет
- Carpal Tunnel SyndromeДокумент5 страницCarpal Tunnel SyndromeBùi Ngọc Anh HSTCОценок пока нет
- Lower Urinary Tract Symptoms LUTS PDFДокумент24 страницыLower Urinary Tract Symptoms LUTS PDFnuriОценок пока нет
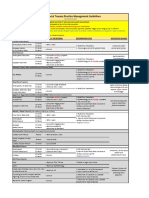
- VUMC Facial Trauma Practice Management GuidelinesДокумент1 страницаVUMC Facial Trauma Practice Management GuidelinesIndra D KristionoОценок пока нет
- 109 Upper Extremity Questions and AnswersДокумент8 страниц109 Upper Extremity Questions and AnswersChioma BenedetteОценок пока нет
- Demo Teaching Physical Health AssessmentДокумент5 страницDemo Teaching Physical Health AssessmentJulie May SuganobОценок пока нет
- Pron 1993Документ10 страницPron 1993Javiera Paz Rios CarmonaОценок пока нет
- Git AnatomyДокумент62 страницыGit AnatomyBimo HarmajiОценок пока нет
- Ent Trauma DanuДокумент52 страницыEnt Trauma Danudanu100% (1)
- Anatomy of Spinal Cord and Spinal Nerves, Reflexes, and Reaction Time and LearningДокумент32 страницыAnatomy of Spinal Cord and Spinal Nerves, Reflexes, and Reaction Time and LearningMickeyОценок пока нет
- (PhysioB) Motor System II - Dr. Vila (Lea Pacis)Документ5 страниц(PhysioB) Motor System II - Dr. Vila (Lea Pacis)miguel cuevasОценок пока нет
- The Heart Has Several Pacemakers Known As Autonomic FociДокумент1 страницаThe Heart Has Several Pacemakers Known As Autonomic FociAnonymous mLYupGyNОценок пока нет
- Ergonomics ExercisesДокумент1 страницаErgonomics Exercisesgeetesh_sОценок пока нет
- Kuliah 3 - Fisiologi Sistem Muskuloskeletal (Dr. Adelia Handoko)Документ36 страницKuliah 3 - Fisiologi Sistem Muskuloskeletal (Dr. Adelia Handoko)Linda ayuОценок пока нет
- Stroke HandoutДокумент5 страницStroke HandoutAdebayo Tob AdeyinkaОценок пока нет