Вам также может понравиться
- Antibiotics (Role and Abuse) 2016Документ35 страницAntibiotics (Role and Abuse) 2016Mohd Johari Mohd ShafuwanОценок пока нет
- Childhood Immunization OWДокумент24 страницыChildhood Immunization OWMohd Johari Mohd ShafuwanОценок пока нет
- Connective Tissue DiseasesДокумент22 страницыConnective Tissue DiseasesMohd Johari Mohd ShafuwanОценок пока нет
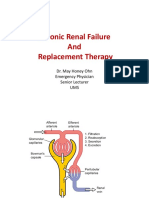
- Chronic Renal Failure and Renal Replacement TherapyДокумент76 страницChronic Renal Failure and Renal Replacement TherapyMohd Johari Mohd ShafuwanОценок пока нет
- Lo 5 and 6Документ32 страницыLo 5 and 6Mohd Johari Mohd ShafuwanОценок пока нет
- Acute Liver FailureДокумент24 страницыAcute Liver FailureMohd Johari Mohd ShafuwanОценок пока нет
- l8 Management of Perianal Pain and ConditionsДокумент51 страницаl8 Management of Perianal Pain and ConditionsMohd Johari Mohd ShafuwanОценок пока нет
- 2016 PE2 TheoryДокумент21 страница2016 PE2 TheoryMohd Johari Mohd ShafuwanОценок пока нет
- Liver Cirrhosis: Etiology Pathogenesis Clinical Features Management PrognosisДокумент35 страницLiver Cirrhosis: Etiology Pathogenesis Clinical Features Management PrognosisMohd Johari Mohd ShafuwanОценок пока нет
- Antibiotics (Role and Abuse)Документ35 страницAntibiotics (Role and Abuse)Mohd Johari Mohd ShafuwanОценок пока нет
- Abg InterpretationДокумент1 страницаAbg InterpretationMohd Johari Mohd ShafuwanОценок пока нет
- Avascular NecrosisДокумент41 страницаAvascular NecrosisMohd Johari Mohd Shafuwan100% (1)
- Chest Tube, Urinary Catheter, Ryles Tube InsertionДокумент60 страницChest Tube, Urinary Catheter, Ryles Tube InsertionMohd Johari Mohd ShafuwanОценок пока нет
- PruritusДокумент9 страницPruritusMohd Johari Mohd ShafuwanОценок пока нет
- Health Promotion LO4Документ41 страницаHealth Promotion LO4Mohd Johari Mohd ShafuwanОценок пока нет
- Health Promotion LO1&2Документ24 страницыHealth Promotion LO1&2Mohd Johari Mohd ShafuwanОценок пока нет
- Adult Immunisation Guideline 2nd Edition 2014Документ184 страницыAdult Immunisation Guideline 2nd Edition 2014Mohd Johari Mohd ShafuwanОценок пока нет
- Open FracturesДокумент43 страницыOpen FracturesMohd Johari Mohd ShafuwanОценок пока нет
- l8 Diabetes Melitus in PregnancyДокумент23 страницыl8 Diabetes Melitus in PregnancyMohd Johari Mohd ShafuwanОценок пока нет
- SchizophreniaДокумент67 страницSchizophreniaHazirah Mokhtar100% (1)
- SGD 10Документ38 страницSGD 10Mohd Johari Mohd ShafuwanОценок пока нет
- ISNCSCI Exam FormДокумент2 страницыISNCSCI Exam FormMónica CruzОценок пока нет
- Diabetes Mellitus in District HospitalДокумент30 страницDiabetes Mellitus in District HospitalMohd Johari Mohd ShafuwanОценок пока нет
- Hypertension in The District HospitalДокумент23 страницыHypertension in The District HospitalMohd Johari Mohd ShafuwanОценок пока нет
- Case Presentation 2Документ42 страницыCase Presentation 2Mohd Johari Mohd ShafuwanОценок пока нет
- Manage UA/NSTEMI Guideline 2011Документ62 страницыManage UA/NSTEMI Guideline 2011Mohd RafiОценок пока нет
- Dengue Fever in Malaysia - Fadhila & NadiahДокумент11 страницDengue Fever in Malaysia - Fadhila & NadiahJacklyn NgОценок пока нет
- Ecg Basics Part 1Документ78 страницEcg Basics Part 1Mohd Johari Mohd ShafuwanОценок пока нет
- Normal ECGДокумент63 страницыNormal ECGMohd Johari Mohd ShafuwanОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Ferrets Oncology-MainДокумент26 страницFerrets Oncology-MainJOAQUINALONZOPEREIRAОценок пока нет
- Comprehensive Genomic Profiling at IlluminaДокумент23 страницыComprehensive Genomic Profiling at IlluminaSaulius BarauskasОценок пока нет
- ASCCP Management Guidelines - August 2014 PDFДокумент24 страницыASCCP Management Guidelines - August 2014 PDFAnita BlazevskaОценок пока нет
- About Soft Tissue Sarcoma: Overview and TypesДокумент10 страницAbout Soft Tissue Sarcoma: Overview and TypesPaulo CesarОценок пока нет
- Ekstrak Kulit Buah Naga Super Merah Sebagai Anti-Kanker PayudaraДокумент5 страницEkstrak Kulit Buah Naga Super Merah Sebagai Anti-Kanker PayudaraWildatul Latifah IIОценок пока нет
- Chemotherapy Dont Cure CancerДокумент2 страницыChemotherapy Dont Cure CancerDr See Kin HaiОценок пока нет
- Exam 4Документ10 страницExam 4pauchanmnlОценок пока нет
- Pathoma - Chapter 13 - FemaleGenitalSysДокумент17 страницPathoma - Chapter 13 - FemaleGenitalSysshanuddinОценок пока нет
- 10 Carcinomatoza PeritonealaДокумент9 страниц10 Carcinomatoza PeritonealaGabriela MilitaruОценок пока нет
- Management of Incidental Pancreatic Cysts: A White Paper of The ACR Incidental Findings CommitteeДокумент13 страницManagement of Incidental Pancreatic Cysts: A White Paper of The ACR Incidental Findings CommitteeSole GonzalezОценок пока нет
- National Cancer Control Programmes in ThailandДокумент93 страницыNational Cancer Control Programmes in ThailandIndonesian Journal of CancerОценок пока нет
- Case Rreport Ameloblastoma English1Документ13 страницCase Rreport Ameloblastoma English1Sisca Dwi AgustinaОценок пока нет
- Psa TestДокумент2 страницыPsa Testmeddco healthcareОценок пока нет
- Giant Cell TumorДокумент35 страницGiant Cell TumorHestikrnОценок пока нет
- A Second-Generation Dendritic Cell Cancer Vaccine Preparing To ShineДокумент19 страницA Second-Generation Dendritic Cell Cancer Vaccine Preparing To Shinebiggercapital100% (5)
- Consensus On The Pathological Definition and Classification of Poorly Cohesive Gastric CarcinomaДокумент9 страницConsensus On The Pathological Definition and Classification of Poorly Cohesive Gastric CarcinomaMariangel FloresОценок пока нет
- Benign Breast DiseaseДокумент48 страницBenign Breast DiseaseNabighah ZukriОценок пока нет
- FNA Biopsy Thyroid Nodules BrochureДокумент2 страницыFNA Biopsy Thyroid Nodules BrochureAndreeaBraduОценок пока нет
- CCSP GuidelinesДокумент42 страницыCCSP GuidelinesAzhagendranОценок пока нет
- Frozen SectionДокумент34 страницыFrozen SectionSnigdha Sinha100% (1)
- Klasifikasi NeoplasmaДокумент22 страницыKlasifikasi Neoplasmaoscar putraОценок пока нет
- Understanding Breast Cancer StagesДокумент7 страницUnderstanding Breast Cancer StagesShyamol Bose0% (1)
- Daftar Pustaka: of Nusring Concept, Process, and Practice 8 TH Edition. New JerseyДокумент6 страницDaftar Pustaka: of Nusring Concept, Process, and Practice 8 TH Edition. New JerseyEpiTa ListyaОценок пока нет
- Appendix C2 Cover Letter ASUBARДокумент2 страницыAppendix C2 Cover Letter ASUBARRuel Vincent AsubarОценок пока нет
- Bladder CancerДокумент19 страницBladder Cancervishnu100% (1)
- LumpectomyДокумент4 страницыLumpectomyvicenteturasОценок пока нет
- Stress Levels Affect Cancer Patients' Coping Mechanisms Based on Cancer Therapy ManagementДокумент15 страницStress Levels Affect Cancer Patients' Coping Mechanisms Based on Cancer Therapy ManagementKeke ManteroОценок пока нет
- MebendazoleДокумент4 страницыMebendazoleJames CullumberОценок пока нет
- Mutations in Brain TumorsДокумент13 страницMutations in Brain TumorsNadia HristovaОценок пока нет
- Cancer Awareness, Safety WeekДокумент47 страницCancer Awareness, Safety WeekpradeepОценок пока нет