Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
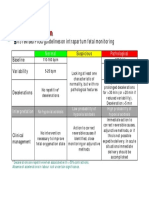
- CTG Classification PDFДокумент1 страницаCTG Classification PDFganotОценок пока нет
- Center - Ranking v1Документ132 страницыCenter - Ranking v1YL LYОценок пока нет
- 2016 PSSI-5 PsychologicalAssessmentДокумент8 страниц2016 PSSI-5 PsychologicalAssessmentLitzaОценок пока нет
- Definition of Aquatic ExerciseДокумент3 страницыDefinition of Aquatic Exercisevenkata ramakrishnaiahОценок пока нет
- Dr. Shoeb MujawarДокумент4 страницыDr. Shoeb Mujawarmeena syedОценок пока нет
- Tes 3Документ1 страницаTes 3M Fadli FahdurohmanОценок пока нет
- Welcome Letter For FamiliesДокумент3 страницыWelcome Letter For FamiliesChild and Family InstituteОценок пока нет
- Cleft Lip & PalateДокумент24 страницыCleft Lip & PalateBheru Lal0% (1)
- 04 Disorders 2Документ27 страниц04 Disorders 2Dayan CabrigaОценок пока нет
- Diagnosis:: Department of TraumatologyДокумент7 страницDiagnosis:: Department of TraumatologyCroitort53100% (1)
- Prurigo Nodularis: Sibylle Eigelshoven, Bernhard HomeyДокумент16 страницPrurigo Nodularis: Sibylle Eigelshoven, Bernhard HomeyLuciana Maria NascimentoОценок пока нет
- Computational BioengineeringДокумент480 страницComputational Bioengineeringscribd990Оценок пока нет
- Management of Head InjuryДокумент27 страницManagement of Head InjuryrosybashОценок пока нет
- Drug Study - CaДокумент3 страницыDrug Study - Casaint_ronald8Оценок пока нет
- Aflac Claim FormДокумент7 страницAflac Claim FormThomas Barrett100% (2)
- ISAPS News Letter 2018Документ52 страницыISAPS News Letter 2018Man Koon Suh, M.D.Оценок пока нет
- William GlasserДокумент3 страницыWilliam GlasserMyrelleОценок пока нет
- NCP - BronchopneumoniaДокумент11 страницNCP - BronchopneumoniaMaria Ivy Mendoza100% (1)
- Dialysis Disequilibrium Syndrome in Neurointensive Care Unit - The Benefit of Intracranial Pressure MonitoringДокумент2 страницыDialysis Disequilibrium Syndrome in Neurointensive Care Unit - The Benefit of Intracranial Pressure Monitoringsatyagraha84Оценок пока нет
- Asia Pacific Occupational Therapy Congress ProgrammeДокумент8 страницAsia Pacific Occupational Therapy Congress ProgrammeRLedgerdОценок пока нет
- JAAOS - Volume 11 - Issue 05 September & October 2003Документ83 страницыJAAOS - Volume 11 - Issue 05 September & October 2003kenthepaОценок пока нет
- Sigmund Freud Essay - WordДокумент9 страницSigmund Freud Essay - Wordapi-2493113410% (1)
- .My - Your Skin Specialist Petaling JayaДокумент7 страниц.My - Your Skin Specialist Petaling JayaMyClinicОценок пока нет
- Medical Records in Family PracticeДокумент22 страницыMedical Records in Family PracticenurfadillahОценок пока нет
- Buku Objektif Praktek Klinis Keperawatan Iv (PKK Iv) : Nama MahasiswaДокумент53 страницыBuku Objektif Praktek Klinis Keperawatan Iv (PKK Iv) : Nama MahasiswaGamaliel Kevin WinarnoОценок пока нет
- Sonopuls 492Документ17 страницSonopuls 492maroun machaalanyОценок пока нет
- Test Taking StrategiesДокумент85 страницTest Taking StrategiesNyjil Patrick Basilio ColumbresОценок пока нет
- Code of EthicsДокумент27 страницCode of EthicsnaomiОценок пока нет
- Pneumonia Journal PediatricsДокумент14 страницPneumonia Journal PediatricstrialqwОценок пока нет
- Muscle GuardingДокумент3 страницыMuscle GuardingRomeo OpaonОценок пока нет