Вам также может понравиться
- Generic Name T Rade Name Classification Diltiazem Cardizem Antianginals, AntiarrhythmicsДокумент1 страницаGeneric Name T Rade Name Classification Diltiazem Cardizem Antianginals, AntiarrhythmicsChristopher LeeОценок пока нет
- Lab 5 Diabetes InsipidusДокумент6 страницLab 5 Diabetes InsipidusLisa EkapratiwiОценок пока нет
- ACS SchematicДокумент2 страницыACS Schematicswish27Оценок пока нет
- NSTEMIДокумент33 страницыNSTEMIwaazalimahwahidОценок пока нет
- NSTEMI Case PresentationДокумент24 страницыNSTEMI Case PresentationMHIEMHOIОценок пока нет
- Case 7 ResultsДокумент14 страницCase 7 ResultsRegia putri ellandaОценок пока нет
- Introduction - MIДокумент10 страницIntroduction - MIkhimiiiОценок пока нет
- Case 1 - Pneumonia (Final)Документ4 страницыCase 1 - Pneumonia (Final)Joegie ArioОценок пока нет
- Chronic GlomerulonephritisДокумент8 страницChronic GlomerulonephritisDaniel CornerОценок пока нет
- HCVDДокумент5 страницHCVDkhrizaleehОценок пока нет
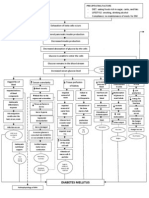
- Pa Tho Physiology of Diabetes MellitusДокумент3 страницыPa Tho Physiology of Diabetes MellitusPong's Teodoro SalvadorОценок пока нет
- Hypertension Pathophysiology and Treatment PDFДокумент6 страницHypertension Pathophysiology and Treatment PDFBella TogasОценок пока нет
- Generic Name Therapeutic Classification Pharmacologic ClassificationДокумент3 страницыGeneric Name Therapeutic Classification Pharmacologic ClassificationAnselle CasilОценок пока нет
- Addison'sДокумент4 страницыAddison'sKoRnflakesОценок пока нет
- Small Bowel ObstructionДокумент2 страницыSmall Bowel ObstructionSrividya PushpalaОценок пока нет
- NCP - Risk For Other-Directed ViolenceДокумент2 страницыNCP - Risk For Other-Directed ViolenceKasandra Dawn Moquia BerisoОценок пока нет
- Hypertensive Cardiovascular DiseaseДокумент16 страницHypertensive Cardiovascular DiseaseTintin Ponciano100% (1)
- Pa Tho Physiology of ParkinsonДокумент2 страницыPa Tho Physiology of Parkinsoncuriosity_killsОценок пока нет
- NURSING CARE PLAN ASSESSMENT FOR CONFUSED PATIENT ON HEMODIALYSISДокумент3 страницыNURSING CARE PLAN ASSESSMENT FOR CONFUSED PATIENT ON HEMODIALYSISgagandipkS100% (1)
- V. Pathophysiology Modifiable: Non - ModifiableДокумент2 страницыV. Pathophysiology Modifiable: Non - ModifiableMary Grace BanezОценок пока нет
- AcknowledgementДокумент9 страницAcknowledgementjhzenОценок пока нет
- Gastritis Types, Causes, Symptoms and TreatmentДокумент17 страницGastritis Types, Causes, Symptoms and TreatmentSri Wahyuni HarliОценок пока нет
- CAP Pneumonia CaseДокумент46 страницCAP Pneumonia CaseMatty FelОценок пока нет
- Cva-Hypertension-Case-Analysis-Group-I FinalДокумент59 страницCva-Hypertension-Case-Analysis-Group-I FinalVhince Norben PiscoОценок пока нет
- Upper Gastrointestinal BleedingДокумент69 страницUpper Gastrointestinal Bleedingeliza luisОценок пока нет
- Buerger Disease Diagnosis and TreatmentДокумент10 страницBuerger Disease Diagnosis and Treatmentautorace007Оценок пока нет
- LA Myxoma Case PresentationДокумент34 страницыLA Myxoma Case PresentationWiwik Puji LestariОценок пока нет
- Renal Case Study Final1Документ41 страницаRenal Case Study Final1api-202881815100% (1)
- Tatz Pa ToolДокумент23 страницыTatz Pa Toolian_mendoza_3Оценок пока нет
- Osteoarthritis 1583-170210113823Документ34 страницыOsteoarthritis 1583-170210113823Angelic khanОценок пока нет
- Nstemi: How To Risk Stratify?Документ32 страницыNstemi: How To Risk Stratify?dhannibernadetОценок пока нет
- Acute TonsillitisДокумент7 страницAcute TonsillitisMichael HostiadiОценок пока нет
- Recurrent PAF Case StudyДокумент3 страницыRecurrent PAF Case StudyDanae Kristina Natasia BangkanОценок пока нет
- Nursing Care Plan for Impaired Bowel EliminationДокумент4 страницыNursing Care Plan for Impaired Bowel EliminationMara Jon Ocden CasibenОценок пока нет
- C191W003 Control Bleeding and Hypovolemic ShockДокумент51 страницаC191W003 Control Bleeding and Hypovolemic ShockEmad Hussien Haj-AbdullaОценок пока нет
- BSN4D-SG2 DM Type2Документ201 страницаBSN4D-SG2 DM Type2Charisse CaydanОценок пока нет
- 403 Full PDFДокумент10 страниц403 Full PDFKuroto YoshikiОценок пока нет
- Case Study Worksheet EndocarditisДокумент6 страницCase Study Worksheet EndocarditisSharlee StoneОценок пока нет
- Pat 2 Medsurg1Документ20 страницPat 2 Medsurg1api-300849832Оценок пока нет
- Head Nurse Experience (Staffing)Документ3 страницыHead Nurse Experience (Staffing)Abigail BrillantesОценок пока нет
- Stomach CancerДокумент7 страницStomach CancerSyazmin KhairuddinОценок пока нет
- STEMI anteroseptalДокумент42 страницыSTEMI anteroseptalWarren LieОценок пока нет
- Schematic Diagram: Signs and Symptoms: Headache, Unconsciousness, Nausea and Vomiting, Visual DisturbancesДокумент3 страницыSchematic Diagram: Signs and Symptoms: Headache, Unconsciousness, Nausea and Vomiting, Visual DisturbancesJosett RomanoОценок пока нет
- Management of Acute Gastroenteritis in ChildrenДокумент14 страницManagement of Acute Gastroenteritis in ChildrenYayaОценок пока нет
- Managing Hypertension to Prevent ComplicationsДокумент10 страницManaging Hypertension to Prevent ComplicationsArabylle Maranca AbuelОценок пока нет
- Clinical Worksheet for Stroke PatientДокумент6 страницClinical Worksheet for Stroke PatientJackie GriffisОценок пока нет
- NCP HemorrhoidsДокумент2 страницыNCP Hemorrhoidsnurse_yramenaj0% (1)
- Nursing Care Plan for Acute Pain PatientДокумент2 страницыNursing Care Plan for Acute Pain PatientAnni BarbaОценок пока нет
- Cefazolin for Skin and Moderate Bacterial InfectionsДокумент5 страницCefazolin for Skin and Moderate Bacterial InfectionsJann Zaniel Allayne RiОценок пока нет
- General ObjectivesДокумент1 страницаGeneral ObjectivesErwin DegraciaОценок пока нет
- Appendicitis NCPДокумент5 страницAppendicitis NCPEarl Joseph DezaОценок пока нет
- CnsДокумент15 страницCnsArun GeorgeОценок пока нет
- DimenhydrinateДокумент2 страницыDimenhydrinateNinoska Garcia-Ortiz100% (1)
- Fracture Closed Complete Displaced Middle Third Femur Right Secondary To FallДокумент102 страницыFracture Closed Complete Displaced Middle Third Femur Right Secondary To FallRaidis PangilinanОценок пока нет
- Bacls PDFДокумент23 страницыBacls PDFAngelo Domingo0% (1)
- Diabetes Mellitus - Diabetic KetoacidosisДокумент21 страницаDiabetes Mellitus - Diabetic KetoacidosisJamil Lorca100% (5)
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Problem-based Approach to Gastroenterology and HepatologyОт EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisОценок пока нет
- STEMIДокумент28 страницSTEMIGP HMHОценок пока нет
- NSTEMIДокумент31 страницаNSTEMISri MegawatiОценок пока нет
- Wilms' Tumor Survival Rates and Max Wilms' BackgroundДокумент20 страницWilms' Tumor Survival Rates and Max Wilms' BackgroundFitriya SyaifuddinОценок пока нет
- Geriatric 2 PDFДокумент52 страницыGeriatric 2 PDFFitriya SyaifuddinОценок пока нет
- Obat PatenqДокумент14 страницObat PatenqFitriya SyaifuddinОценок пока нет
- Pi Is 0090429514003781Документ4 страницыPi Is 0090429514003781Fitriya SyaifuddinОценок пока нет
- Final Trauma11Документ15 страницFinal Trauma11Milo PingОценок пока нет
- Daftar PustakaДокумент1 страницаDaftar PustakaFitriya SyaifuddinОценок пока нет
- Intestinal ObstructionДокумент10 страницIntestinal Obstructionapi-3712326Оценок пока нет
- Cardiac Rehabilitation Case Study ExplainedДокумент20 страницCardiac Rehabilitation Case Study Explainedعادل خليلОценок пока нет
- Emergency Medicine 1st Edition - DR - Waleed (101 Papers)Документ101 страницаEmergency Medicine 1st Edition - DR - Waleed (101 Papers)Mokhtar Moh100% (1)
- Basic Life Support and Advanced Cardiac Life Support: Knowledge of Medical Students in New DelhiДокумент9 страницBasic Life Support and Advanced Cardiac Life Support: Knowledge of Medical Students in New DelhiSriatiОценок пока нет
- Electrode Placement: Midclavicular LineДокумент4 страницыElectrode Placement: Midclavicular LineJeneleth DayaodaoОценок пока нет
- DYSRHYTHMIAS (A.k.a. Arrhythmias) Disorders in TheДокумент3 страницыDYSRHYTHMIAS (A.k.a. Arrhythmias) Disorders in TheDarell M. Book100% (1)
- Course Exercise - ACLS Precourse Self-Assessment and Precourse Work, InternationДокумент3 страницыCourse Exercise - ACLS Precourse Self-Assessment and Precourse Work, InternationUnkakb 20Оценок пока нет
- How To Detect Long QT in A Heartbeat - Clinical ViewДокумент9 страницHow To Detect Long QT in A Heartbeat - Clinical ViewAlberto MHОценок пока нет
- The Cardiac Cycle and The Physiologic Basis of Left Ventricular Contraction, Ejection, Relaxation, and FillingДокумент13 страницThe Cardiac Cycle and The Physiologic Basis of Left Ventricular Contraction, Ejection, Relaxation, and FillingFanindya HadamuОценок пока нет
- Arritmias en El EmbarazoДокумент10 страницArritmias en El EmbarazoJuan Soto FarfanОценок пока нет
- Philips IE33 XMatrix Ecocardiography System Ultrasound MachineДокумент16 страницPhilips IE33 XMatrix Ecocardiography System Ultrasound MachineHAITHM MURSHEDОценок пока нет
- Adult 3 FinalДокумент29 страницAdult 3 Finalأبوأحمد الحكيم100% (1)
- CVS-01 Examination & Short CasesДокумент9 страницCVS-01 Examination & Short Casesem khanОценок пока нет
- Dr. Ika Prasetya WijayaДокумент31 страницаDr. Ika Prasetya Wijayabidang keperawatanОценок пока нет
- Cardiac Five YearsДокумент31 страницаCardiac Five Yearsdileepkumar.duhs4817Оценок пока нет
- P Wave AbnormalitiesДокумент9 страницP Wave Abnormalitieswilliam atmadjiОценок пока нет
- RhythmДокумент8 страницRhythmparkmickyboo100% (1)
- Development of The HeartДокумент19 страницDevelopment of The HeartYusuf UmarОценок пока нет
- Cardiovascular System Short Answer QuestionsДокумент10 страницCardiovascular System Short Answer QuestionsPrateek BhasinОценок пока нет
- Speaker: Maj YS Swapna Sudha Chair Person: Maj Swapna Dharmaji Moderator: Col S.SenguptaДокумент33 страницыSpeaker: Maj YS Swapna Sudha Chair Person: Maj Swapna Dharmaji Moderator: Col S.SenguptaSudha Kiran100% (1)
- KKH Baby Bear Book 3rd EditionДокумент672 страницыKKH Baby Bear Book 3rd EditionJonathan TayОценок пока нет
- Internal Med Board Review Course BK 2013-2014Документ564 страницыInternal Med Board Review Course BK 2013-2014Akash Bhatnagar100% (1)
- Test Bank For Ecg Essentials of Electrocardiography 1st Edition by SotoДокумент9 страницTest Bank For Ecg Essentials of Electrocardiography 1st Edition by Sotopamelachavezbawyoemckf100% (26)
- Cardiology Nurse ResumeДокумент6 страницCardiology Nurse Resumecnkokuekg100% (1)
- Coronary Angiography: A Continuing Education ProgramДокумент71 страницаCoronary Angiography: A Continuing Education ProgramVincha R LuqmanОценок пока нет
- Med TagДокумент23 страницыMed TagClarissa GuifayaОценок пока нет
- A Nursing HandoverДокумент3 страницыA Nursing HandoverZaidan YusufОценок пока нет
- Lesson Plan On CPRДокумент3 страницыLesson Plan On CPRanimesh pandaОценок пока нет
- 4.17 Tighe Mitral Valve Prostheses PDFДокумент60 страниц4.17 Tighe Mitral Valve Prostheses PDFBrie DanielОценок пока нет
- Acls Version B QuizДокумент9 страницAcls Version B QuizRokunuz Jahan Rudro0% (1)
- Achaiki - Iatriki - April-June 2020-1Документ52 страницыAchaiki - Iatriki - April-June 2020-1NIKOLAOS SYRMOSОценок пока нет