Вам также может понравиться
- The Oral-Systemic Connection: Understanding the Relationship Between Periodontal Disease and Systemic HealthДокумент25 страницThe Oral-Systemic Connection: Understanding the Relationship Between Periodontal Disease and Systemic HealthAditya ZulfikarОценок пока нет
- Denture Stomatitis KP UNissula Mei 2016Документ53 страницыDenture Stomatitis KP UNissula Mei 2016Aditya ZulfikarОценок пока нет
- REBASING & RELINING DENTURES COMPLETELYДокумент18 страницREBASING & RELINING DENTURES COMPLETELYAditya ZulfikarОценок пока нет
- KP Lesi Pre Kanker Kanker Dan Efek Terapi Kanker Rongga MulutДокумент58 страницKP Lesi Pre Kanker Kanker Dan Efek Terapi Kanker Rongga MulutAditya ZulfikarОценок пока нет
- Dok Rama (Functional Appliance)Документ36 страницDok Rama (Functional Appliance)Aditya ZulfikarОценок пока нет
- Dok Yusuf (Ekstraoral Radiography)Документ72 страницыDok Yusuf (Ekstraoral Radiography)Aditya ZulfikarОценок пока нет
- Pengaruh Terapi CA Pada Rongga MulutДокумент24 страницыPengaruh Terapi CA Pada Rongga MulutAditya ZulfikarОценок пока нет
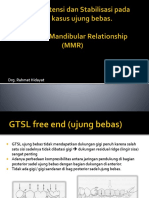
- Dok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRДокумент53 страницыDok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRAditya ZulfikarОценок пока нет
- Dok Yusuf (Ekstraoral Radiography)Документ72 страницыDok Yusuf (Ekstraoral Radiography)Aditya ZulfikarОценок пока нет
- DRG Ade MSLH Elderely MHSWДокумент36 страницDRG Ade MSLH Elderely MHSWAditya ZulfikarОценок пока нет
- Periodontal Disease and Systemic Health ConnectionДокумент25 страницPeriodontal Disease and Systemic Health ConnectionAditya ZulfikarОценок пока нет
- GINGIVAL Disease KulpakДокумент61 страницаGINGIVAL Disease KulpakAditya ZulfikarОценок пока нет
- Komplikasi AlДокумент29 страницKomplikasi AlAditya ZulfikarОценок пока нет
- Komplikasi AlДокумент29 страницKomplikasi AlAditya ZulfikarОценок пока нет
- Dental AnatomyДокумент61 страницаDental AnatomyAditya ZulfikarОценок пока нет
- Dok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRДокумент53 страницыDok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRAditya ZulfikarОценок пока нет
- DRG Ade MSLH Elderely MHSWДокумент36 страницDRG Ade MSLH Elderely MHSWAditya ZulfikarОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5782)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Arslan CVДокумент18 страницArslan CVAwais NaeemОценок пока нет
- Copyright WorksheetДокумент3 страницыCopyright WorksheetJADEN GOODWINОценок пока нет
- 1000 Plus Psychiatry MCQ Book DranilkakunjeДокумент141 страница1000 Plus Psychiatry MCQ Book Dranilkakunjethelegend 20220% (1)
- DLP - Q1 - Week 5Документ7 страницDLP - Q1 - Week 5IVY MALEОценок пока нет
- Chapter 7 - Application of Dielectric Spectroscopy To The Characterization of FAME in BiodieselДокумент10 страницChapter 7 - Application of Dielectric Spectroscopy To The Characterization of FAME in BiodieselAlfonso MartínezОценок пока нет
- Face ReadingДокумент31 страницаFace ReadingGnana Guru100% (4)
- ME EngRW 11 Q3 0401 PS NarrationДокумент29 страницME EngRW 11 Q3 0401 PS NarrationKyle OrlanesОценок пока нет
- Database Design Term Project 1Документ3 страницыDatabase Design Term Project 1MuskanОценок пока нет
- Emergency procedures for shipboard fire suppression systemsДокумент1 страницаEmergency procedures for shipboard fire suppression systemsImmorthalОценок пока нет
- Very Good, Course Steered, Speed Rung, Engine Configuration, You Have the ConДокумент5 страницVery Good, Course Steered, Speed Rung, Engine Configuration, You Have the ConRoger Medallon Bag-aoОценок пока нет
- Ministry of Fisheries Report Into Hoki FisheriesДокумент141 страницаMinistry of Fisheries Report Into Hoki FisheriesNewshubОценок пока нет
- Asme Sec 5 TofdДокумент6 страницAsme Sec 5 TofdarsalanhaqОценок пока нет
- Field Trip 2 - Coreslab Structures Inc Essay - FinalДокумент11 страницField Trip 2 - Coreslab Structures Inc Essay - Finalmmg009Оценок пока нет
- Electric Expansion Valve: Type ETS 12.5 - ETS 400Документ18 страницElectric Expansion Valve: Type ETS 12.5 - ETS 400Mustafa MouradОценок пока нет
- English for Public Information LK 1Документ7 страницEnglish for Public Information LK 1jauhar muttaqinОценок пока нет
- Bells and WhistlesДокумент2 страницыBells and Whistlesapi-265536295Оценок пока нет
- School Form 1 SF 1 10Документ6 страницSchool Form 1 SF 1 10ALEX SARAOSOSОценок пока нет
- FBAI Final ReportДокумент14 страницFBAI Final ReportSrishti JoshiОценок пока нет
- Kofax Digital Mailroom Webinar IDC Slides v4Документ16 страницKofax Digital Mailroom Webinar IDC Slides v4hteran28100% (2)
- Programmable Logic Controller (PLC)Документ19 страницProgrammable Logic Controller (PLC)Jason Sonido88% (8)
- Shaikh Khalifa Bin Zayed Al-Nahyan Medical Dental College LahoreДокумент1 страницаShaikh Khalifa Bin Zayed Al-Nahyan Medical Dental College LahoreHamad GulОценок пока нет
- Pushover Analysis As Per EC8Документ23 страницыPushover Analysis As Per EC8mihaitimofteОценок пока нет
- Autism and Autism Spectrum Disorder Medical Hypothesis For Parasites Influencing AutismДокумент3 страницыAutism and Autism Spectrum Disorder Medical Hypothesis For Parasites Influencing AutismCATHYОценок пока нет
- 2023 Imec Wind Symphony ProgramДокумент16 страниц2023 Imec Wind Symphony Programapi-583612673Оценок пока нет
- UTOPIAvs DYSTOPIAДокумент17 страницUTOPIAvs DYSTOPIAzairaguenperaltaОценок пока нет
- Environment - Parallel Session - Jo Rowena GarciaДокумент26 страницEnvironment - Parallel Session - Jo Rowena GarciaAsian Development Bank ConferencesОценок пока нет
- Nexus FP PDFДокумент48 страницNexus FP PDFPeter MkamaОценок пока нет
- Prelim Lesson 2 Global EconomyДокумент26 страницPrelim Lesson 2 Global EconomyJANETH SATRAINОценок пока нет
- PLTW AR MechanismDemonstrationPowerPointДокумент29 страницPLTW AR MechanismDemonstrationPowerPointAbdulsalam OmotoshoОценок пока нет
- TOJan Feb 16Документ40 страницTOJan Feb 16kumararajОценок пока нет