Вам также может понравиться
- Non-Invasive Cardiac ImagingДокумент9 страницNon-Invasive Cardiac Imagingoddone_outОценок пока нет
- Cardiology EssentialsДокумент396 страницCardiology Essentialsanna100% (16)
- Study of Pediatric Congenital Cardiac Malformations by EchocardiographyДокумент23 страницыStudy of Pediatric Congenital Cardiac Malformations by EchocardiographyRana Abd AlmugeethОценок пока нет
- Algorithm-ACLS ACS 200806 1Документ1 страницаAlgorithm-ACLS ACS 200806 1Kavya Shree100% (1)
- HEARTДокумент14 страницHEARTNag Mallesh RaoОценок пока нет
- MapseДокумент6 страницMapseRaul GascueñaОценок пока нет
- CCD Guidelines 2023Документ123 страницыCCD Guidelines 2023Cuong Nguyen Vu TheОценок пока нет
- Prosth ValvesДокумент74 страницыProsth ValvesRavi ZoreОценок пока нет
- Left Ventricular Hypertrophy: Detection, Significance and TreatmentДокумент27 страницLeft Ventricular Hypertrophy: Detection, Significance and TreatmentKudor Szabadi ZoltánОценок пока нет
- Simple Office SpirometryДокумент42 страницыSimple Office SpirometryRoberto Merza III100% (4)
- Sinus Node DysfunctionДокумент11 страницSinus Node DysfunctionVasishta Nadella100% (1)
- Quantification of Severity of Mitral Regurgitation With The New ASE GuidelinesДокумент20 страницQuantification of Severity of Mitral Regurgitation With The New ASE GuidelinesPanfilAlinaОценок пока нет
- Eye Exercises To Improve VisionДокумент4 страницыEye Exercises To Improve VisionVik Shar100% (1)
- Global Longitudinal StrainДокумент7 страницGlobal Longitudinal StrainBinod KumarОценок пока нет
- EKG Crash Course NuRsing 390 SMC - 4Документ57 страницEKG Crash Course NuRsing 390 SMC - 4m1k0e100% (2)
- @ebookmedicin Cardiology Clinics February 2017Документ19 страниц@ebookmedicin Cardiology Clinics February 2017mulyadiОценок пока нет
- Deepika Thacker, Jack Rychik (Auth.), Robert. E Shaddy (Eds.) - Heart Failure in Congenital Heart Disease - From Fetus To Adult (2011, Springer-Verlag London)Документ187 страницDeepika Thacker, Jack Rychik (Auth.), Robert. E Shaddy (Eds.) - Heart Failure in Congenital Heart Disease - From Fetus To Adult (2011, Springer-Verlag London)paul00040Оценок пока нет
- Mitral RegurgitationДокумент6 страницMitral RegurgitationMelfi Triani SiskaОценок пока нет
- Pna 2022Документ49 страницPna 2022MafaldaGomesОценок пока нет
- Pediatric Cardiology LectureДокумент87 страницPediatric Cardiology LectureMena HashemОценок пока нет
- ABSITEДокумент38 страницABSITEVik SharОценок пока нет
- Cardiovascular ExaminationДокумент13 страницCardiovascular ExaminationBitu JaaОценок пока нет
- CARDIAC CYCLE New For StudentДокумент54 страницыCARDIAC CYCLE New For StudentDavi DzikirianОценок пока нет
- Guide To Cathether PDFДокумент224 страницыGuide To Cathether PDFSugeng PrakosoОценок пока нет
- RV Dysfunction - Assessment by EchocardiographyДокумент52 страницыRV Dysfunction - Assessment by EchocardiographyNag Mallesh RaoОценок пока нет
- Echo Facts IndexДокумент3 страницыEcho Facts Indexs336336anl100% (1)
- Diastolic DysfunctionДокумент6 страницDiastolic DysfunctionMarina SecureanuОценок пока нет
- Adult Congenital Heart Disease Board ReviewДокумент79 страницAdult Congenital Heart Disease Board ReviewKhajornsak Som-UnОценок пока нет
- Pacing Week PresentationsДокумент54 страницыPacing Week PresentationsjoejenningsОценок пока нет
- 3 Abdominal Ultrasound Imaging AnatomyДокумент7 страниц3 Abdominal Ultrasound Imaging Anatomyjefaturaimagenologia Hospital NogalarОценок пока нет
- Unit-2 ECG LNRДокумент29 страницUnit-2 ECG LNRNagarajan LОценок пока нет
- Fontan Operation: DR Hussain BuxДокумент62 страницыFontan Operation: DR Hussain BuxMujeeb Ur RehmanОценок пока нет
- Aortic Root FinalДокумент82 страницыAortic Root FinalMustafa KamalОценок пока нет
- Hepatic Vein FlowДокумент14 страницHepatic Vein FlowJORGEОценок пока нет
- DO /VO Relationships: J. L. VincentДокумент8 страницDO /VO Relationships: J. L. VincentLucas Cárcamo SaavedraОценок пока нет
- Surgical Management of Ischemic Heart Disease - An UpdateДокумент48 страницSurgical Management of Ischemic Heart Disease - An UpdateRezwanul Hoque BulbulОценок пока нет
- Atrial Septial DefectДокумент22 страницыAtrial Septial DefectJulie MckinneyОценок пока нет
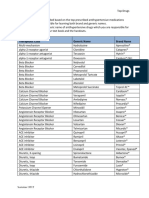
- Top Antihypertensive Drugs Generic-Brand Names PDFДокумент1 страницаTop Antihypertensive Drugs Generic-Brand Names PDFvidbala0% (1)
- Microsoft PowerPoint - ECHOCARDIOGRAPHY IN ADULT CONGENITAL HEART DISEASE PDFДокумент51 страницаMicrosoft PowerPoint - ECHOCARDIOGRAPHY IN ADULT CONGENITAL HEART DISEASE PDFHanafieHeluthОценок пока нет
- DELNIDOДокумент32 страницыDELNIDOsarwansyahОценок пока нет
- Interventional Cardiology Certification Examination Blueprint - American Board of Internal MedicineДокумент3 страницыInterventional Cardiology Certification Examination Blueprint - American Board of Internal MedicineabimorgОценок пока нет
- Pulmonary HypertensionДокумент58 страницPulmonary HypertensionnadiasalimaОценок пока нет
- NCLEX QuestionsДокумент27 страницNCLEX QuestionsAngie MandeoyaОценок пока нет
- Pulmonary SequestrationДокумент15 страницPulmonary SequestrationEmily EresumaОценок пока нет
- EKG in IHDДокумент349 страницEKG in IHDDinhLinh100% (1)
- Congenital Heart DiseaseДокумент74 страницыCongenital Heart DiseaseKeith LajotОценок пока нет
- FinalДокумент56 страницFinalvamshidhОценок пока нет
- Diagnosis and Management of The Neonate With Critical Congenital Heart DiseaseДокумент35 страницDiagnosis and Management of The Neonate With Critical Congenital Heart Diseasemotzco0% (1)
- Austin Journal of Clinical CardiologyДокумент15 страницAustin Journal of Clinical CardiologyAustin Publishing GroupОценок пока нет
- Anatomy of The Ventricular Septal Defect in Congenital Heart DefectДокумент8 страницAnatomy of The Ventricular Septal Defect in Congenital Heart DefectFajar YuniftiadiОценок пока нет
- L-R ShuntДокумент88 страницL-R ShuntnanohaniwiekoОценок пока нет
- AP WindowДокумент13 страницAP WindowHugo GonzálezОценок пока нет
- 2607 FullДокумент94 страницы2607 FullanindiawОценок пока нет
- Basic EP IntervalsДокумент13 страницBasic EP IntervalsdrharoonmohdОценок пока нет
- Mechanisms of Cardiac Arrhythmias From Automatici+Документ24 страницыMechanisms of Cardiac Arrhythmias From Automatici+Malar MannanОценок пока нет
- Mitral RegurgitationДокумент10 страницMitral RegurgitationWalter Saavedra YarlequeОценок пока нет
- Mitral Valve StenosisДокумент2 страницыMitral Valve StenosisSrhi NurhayatiiОценок пока нет
- Practical Guide For The Students Version 2.0Документ906 страницPractical Guide For The Students Version 2.0tejuteju06750% (2)
- Harvesting The Radial ArteryДокумент11 страницHarvesting The Radial ArteryprofarmahОценок пока нет
- Aortic Regurgitation CaseДокумент38 страницAortic Regurgitation CaseIka MagfirahОценок пока нет
- Non Cardiac OpДокумент21 страницаNon Cardiac Opc4ri5Оценок пока нет
- Difficult Weaning From Cardiopulmonary Bypass Final Edit LiaДокумент41 страницаDifficult Weaning From Cardiopulmonary Bypass Final Edit LiaYuri SadewoОценок пока нет
- Fetal ArrhythmiasДокумент18 страницFetal ArrhythmiasKarin Stefanny Muñoz CastilloОценок пока нет
- AGT Applied Anatomy Notes1.1Документ69 страницAGT Applied Anatomy Notes1.1Akshay ChauhanОценок пока нет
- Primary and Secondary CV Prevention - Iman EvanДокумент104 страницыPrimary and Secondary CV Prevention - Iman EvanFikriYTОценок пока нет
- Cardiac SarcoidosisДокумент13 страницCardiac SarcoidosisEmeric Jorge Macedo VendezuОценок пока нет
- APDSДокумент102 страницыAPDSVik SharОценок пока нет
- PH.D Clinical PsychologyДокумент4 страницыPH.D Clinical PsychologyVik SharОценок пока нет
- Fellowship Positions (T32HL129948) : EligibilityДокумент1 страницаFellowship Positions (T32HL129948) : EligibilityVik SharОценок пока нет
- Imagine John LennonДокумент2 страницыImagine John LennonVik SharОценок пока нет
- Types of Clinical QuestionsДокумент4 страницыTypes of Clinical QuestionsVik SharОценок пока нет
- Background Questions Ask For General Knowledge About An Illness, Disease, Condition, ProcessДокумент1 страницаBackground Questions Ask For General Knowledge About An Illness, Disease, Condition, ProcessVik SharОценок пока нет
- Unit ThreeДокумент32 страницыUnit ThreeVik SharОценок пока нет
- Lying Ashwani Kumar Bhardwaj: Monica LewskiДокумент11 страницLying Ashwani Kumar Bhardwaj: Monica LewskiVik SharОценок пока нет
- Ashwani Kumar Bhardwaj Writing Assignment Jan, 19, 2014Документ1 страницаAshwani Kumar Bhardwaj Writing Assignment Jan, 19, 2014Vik SharОценок пока нет
- Atrial FibrillationДокумент20 страницAtrial Fibrillationjack sawdaОценок пока нет
- Class CHAPTER 9 - Circulatory With AnswersДокумент59 страницClass CHAPTER 9 - Circulatory With AnswersSara VinuyaОценок пока нет
- Carpentier Mitral Valve Regurgitation ClasifДокумент45 страницCarpentier Mitral Valve Regurgitation ClasifKudor Szabadi Zoltán100% (1)
- Erp 18 0068Документ17 страницErp 18 0068Jose Ignacio Tarton SisimitОценок пока нет
- Laporan Tutorial Kelompok 1 Skenario 2Документ11 страницLaporan Tutorial Kelompok 1 Skenario 2Anita Dwi srirahayuОценок пока нет
- Pediatric Cardiology Thesis TopicsДокумент4 страницыPediatric Cardiology Thesis Topicspzblktgld100% (2)
- Unit II (B) Intra-Aortic Balloon Pump Counter PulsationДокумент24 страницыUnit II (B) Intra-Aortic Balloon Pump Counter PulsationUmme HabibaОценок пока нет
- 5 Cardiovascular DisordersДокумент4 страницы5 Cardiovascular DisordersChristian Joseph OpianaОценок пока нет
- Atrial Septal Defect: Presented By:-Dr Kunwar Sidharth SaurabhДокумент60 страницAtrial Septal Defect: Presented By:-Dr Kunwar Sidharth SaurabhKunwar Sidharth SaurabhОценок пока нет
- Target BeneficiariesДокумент6 страницTarget BeneficiariesTommy SoleraОценок пока нет
- Cme Acs 2. Stemi (Izzah)Документ36 страницCme Acs 2. Stemi (Izzah)Hakimah K. SuhaimiОценок пока нет
- Clinical QuidДокумент175 страницClinical QuidHassan Al SinanОценок пока нет
- SeminarДокумент34 страницыSeminarMuhammad Faiz Satria WibowoОценок пока нет
- Pathology of HEART - 1Документ175 страницPathology of HEART - 1Abdukadir AzamОценок пока нет
- Strong's EKG Chamber Enlargement - DraftДокумент12 страницStrong's EKG Chamber Enlargement - DraftMonica GonzalezОценок пока нет
- Ebstein's Anomaly: Department of Cardiovascular and Thoracic Surgery Sarit Levinsky Group M1656Документ36 страницEbstein's Anomaly: Department of Cardiovascular and Thoracic Surgery Sarit Levinsky Group M1656Sarit LevinskyОценок пока нет
- Resume CV Houston Based Physician Assistant Cardiology and ER Experience Seeking New Opportunities in Houston Texas Area Post Medical Resume Physician CVДокумент2 страницыResume CV Houston Based Physician Assistant Cardiology and ER Experience Seeking New Opportunities in Houston Texas Area Post Medical Resume Physician CVRick WhitleyОценок пока нет
- Neonatal Cardiac EmergenciesДокумент4 страницыNeonatal Cardiac EmergenciesEstellaОценок пока нет
- Combined Pressure and Flow Measurements To Guide Treatment of Coronary Stenoses PDFДокумент10 страницCombined Pressure and Flow Measurements To Guide Treatment of Coronary Stenoses PDFIsfan RialdyОценок пока нет
- Coils Embolization Use For Coronary Procedures - Cathet Cardio Intervent - 2023 - LohДокумент13 страницCoils Embolization Use For Coronary Procedures - Cathet Cardio Intervent - 2023 - LohEvandro Martins FilhoОценок пока нет
- Shunt Calculation, NICVDДокумент31 страницаShunt Calculation, NICVDNavojit ChowdhuryОценок пока нет
- AHA Elearning - ACLS Precourse Self-Assessment and Precourse WorkДокумент3 страницыAHA Elearning - ACLS Precourse Self-Assessment and Precourse WorkAmmar bushraОценок пока нет