Вам также может понравиться
- Psychopharmacology 2 AntidepressantsДокумент7 страницPsychopharmacology 2 AntidepressantsBea Samonte100% (2)
- Retaining Talent: Replacing Misconceptions With Evidence-Based StrategiesДокумент18 страницRetaining Talent: Replacing Misconceptions With Evidence-Based StrategiesShams Ul HayatОценок пока нет
- Bottoms y Sparks - Legitimacy - and - Imprisonment - Revisited PDFДокумент29 страницBottoms y Sparks - Legitimacy - and - Imprisonment - Revisited PDFrossana gaunaОценок пока нет
- Antidepressant DrugsДокумент41 страницаAntidepressant DrugsSashaKay100% (5)
- Name: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicДокумент16 страницName: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicAnoosha FarooquiОценок пока нет
- Antidepressants AntidepressantsДокумент38 страницAntidepressants AntidepressantsjaneОценок пока нет
- AntidepressantsДокумент5 страницAntidepressantsUm HamoOd100% (2)
- "Serotonin Syndrome Causes HARM": Psychiatry PharamacologyДокумент9 страниц"Serotonin Syndrome Causes HARM": Psychiatry Pharamacologytycobb63100% (4)
- Antidepressant Drugs: Presented By-K.Vinod Dept. of PharmacologyДокумент38 страницAntidepressant Drugs: Presented By-K.Vinod Dept. of PharmacologyVinod GuruОценок пока нет
- Topic 15-1Документ28 страницTopic 15-1riyazadsumaiyajb2003Оценок пока нет
- Antidepresivi - Katzung & Trevor's Pharmacology Examination and Board Review, 9th EditionДокумент7 страницAntidepresivi - Katzung & Trevor's Pharmacology Examination and Board Review, 9th EditionDragutin PetrićОценок пока нет
- Antidepressants (Igor Iezhitsa) Students Copy (ME219)Документ40 страницAntidepressants (Igor Iezhitsa) Students Copy (ME219)Zobayer AhmedОценок пока нет
- نسخة ANTI-ARRHYTHMIC 2Документ28 страницنسخة ANTI-ARRHYTHMIC 2ManWol JangОценок пока нет
- Mechanism of Action: Maois Work by Inhibiting The Activity of Monoamine OxidaseДокумент3 страницыMechanism of Action: Maois Work by Inhibiting The Activity of Monoamine OxidaseHomo SapienОценок пока нет
- Serotonin (5-HT)Документ35 страницSerotonin (5-HT)adeesasaadОценок пока нет
- AntidepressantsДокумент12 страницAntidepressantsSubiVictorОценок пока нет
- AntidepressantsДокумент59 страницAntidepressantsanon_189054600100% (2)
- Antidepressant DrugsДокумент11 страницAntidepressant Drugssuresh patilОценок пока нет
- Antidepressants UOLДокумент85 страницAntidepressants UOLYahya AhmedОценок пока нет
- Drugs For Psyciatric DisordersДокумент19 страницDrugs For Psyciatric Disordersapi-36993610% (1)
- Presentation OutlineДокумент6 страницPresentation OutlineDelniece WilliamsОценок пока нет
- Pharmacology of AntidepressantsДокумент28 страницPharmacology of Antidepressantsحيدر كريم سعيد حمزهОценок пока нет
- Pharmacology 402 February 24, 2010 Mark Hamblin, MD, PHDДокумент54 страницыPharmacology 402 February 24, 2010 Mark Hamblin, MD, PHDKarmila Novianti100% (1)
- Anti Depressants FinalДокумент61 страницаAnti Depressants FinalAuthor Nauman Shad100% (1)
- Antidepreesent AgentsДокумент34 страницыAntidepreesent Agentsmaryamkefahn2003Оценок пока нет
- AntidepressantsДокумент28 страницAntidepressantsakoeljames8543Оценок пока нет
- Antidepressants: Samaiya Mushtaq CHEM 5398Документ33 страницыAntidepressants: Samaiya Mushtaq CHEM 5398Renuga DeviОценок пока нет
- SSRI Effect On DepresionДокумент10 страницSSRI Effect On DepresionWilb ParadaОценок пока нет
- Pharmacology of Mood Stabilizers: DR - Datten Bangun, MSC, SPFK Dept - Farmakologi & Terapetik Fak - Kedokteran Uhn MedanДокумент51 страницаPharmacology of Mood Stabilizers: DR - Datten Bangun, MSC, SPFK Dept - Farmakologi & Terapetik Fak - Kedokteran Uhn MedanFansisca SiallaganОценок пока нет
- Anti Depresan1Документ39 страницAnti Depresan1Akmal SafwanОценок пока нет
- Exposure and Response Prevention TechniqueДокумент9 страницExposure and Response Prevention TechniqueAsghar AmirОценок пока нет
- Sem 4 Lectura 2 Inhibidores de Recaptación de SerotoninaДокумент18 страницSem 4 Lectura 2 Inhibidores de Recaptación de SerotoninaJesús MoraОценок пока нет
- Principles of PharmacologyДокумент29 страницPrinciples of PharmacologyKairy T. CumbalОценок пока нет
- Mechanism Action of DrugsДокумент7 страницMechanism Action of Drugsammaramaryam6463Оценок пока нет
- Pharmacology CNS DrugsДокумент7 страницPharmacology CNS DrugsDavid Hosam100% (1)
- Depression: Types Symptoms Diagnosis Causes TreatmentДокумент32 страницыDepression: Types Symptoms Diagnosis Causes TreatmentThea MallariОценок пока нет
- CNS PharmaДокумент11 страницCNS PharmaRuben ToralloОценок пока нет
- ANTIDEPRESSANTS MaterialДокумент5 страницANTIDEPRESSANTS MaterialxyzОценок пока нет
- Antidepressants MaterialДокумент5 страницAntidepressants MaterialxyzОценок пока нет
- PsychopharmacologyДокумент77 страницPsychopharmacologychachaazkaОценок пока нет
- Antidepressant DrugsДокумент47 страницAntidepressant DrugsOjambo Flavia75% (4)
- Antidepressant DrugsДокумент55 страницAntidepressant Drugsmaheen aurangzaib100% (2)
- B2B Psychopharmacology 2015Документ128 страницB2B Psychopharmacology 2015Soleil DaddouОценок пока нет
- Polyclona/lMonoclonal AB To Serotonin Receptors As Therapeutic Agents.Документ26 страницPolyclona/lMonoclonal AB To Serotonin Receptors As Therapeutic Agents.Dmitri PopovОценок пока нет
- Bms166 Slide Antipsychotic AntidepressantДокумент52 страницыBms166 Slide Antipsychotic AntidepressantErmanto D'PhytoxzОценок пока нет
- Antipsychotic DrugsДокумент6 страницAntipsychotic DrugsNispap Harami RJОценок пока нет
- Psychopamacology PresentationДокумент131 страницаPsychopamacology Presentationsalmalissu0Оценок пока нет
- Antidepressant Juli 2016Документ18 страницAntidepressant Juli 2016NadiarosmaliaОценок пока нет
- Psychotropic DrugsДокумент11 страницPsychotropic DrugscchatrumaОценок пока нет
- Katzung Chapter 30 AntidepressantsДокумент69 страницKatzung Chapter 30 AntidepressantsMeetAndreaОценок пока нет
- Systemic Effects of Histamine and SerotoninДокумент5 страницSystemic Effects of Histamine and SerotoninibrahimОценок пока нет
- Pharmacology of Serotonergic and Central Adrenergic Neurotransmission-Week 6Документ46 страницPharmacology of Serotonergic and Central Adrenergic Neurotransmission-Week 6boboОценок пока нет
- AntipsychoticsДокумент77 страницAntipsychoticsGokulnath MbbsОценок пока нет
- AntidepressantДокумент8 страницAntidepressantKlarasita WibowoОценок пока нет
- The PSYCH MAP ColoredДокумент2 страницыThe PSYCH MAP Coloredcentrino17Оценок пока нет
- Substance Abuse and Toxins - 20120531Документ23 страницыSubstance Abuse and Toxins - 20120531Cindy Van WykОценок пока нет
- AntidepressantsДокумент20 страницAntidepressantsvimalaОценок пока нет
- The Only Two Ways To Raise Brain Serotonin Levels - IHealthTubeДокумент8 страницThe Only Two Ways To Raise Brain Serotonin Levels - IHealthTubekrishanОценок пока нет
- Mechanism and Side Effects of SSRI 1Документ13 страницMechanism and Side Effects of SSRI 1Andika MetrisiawanОценок пока нет
- The Search for Antidepressants - An Integrative View of Drug DiscoveryОт EverandThe Search for Antidepressants - An Integrative View of Drug DiscoveryОценок пока нет
- Mood (Affective) Disorders: To Meet Wikipedia's, This Article or Section May RequireДокумент3 страницыMood (Affective) Disorders: To Meet Wikipedia's, This Article or Section May RequiremengakuОценок пока нет
- Dementia & DeliriumДокумент170 страницDementia & Deliriummengaku0% (1)
- Attention Deficit Hyperactivity DisorderДокумент42 страницыAttention Deficit Hyperactivity DisordermengakuОценок пока нет
- Antipsychotic AgentsДокумент18 страницAntipsychotic AgentsmengakuОценок пока нет
- Antidepressant DrugsДокумент11 страницAntidepressant DrugsmengakuОценок пока нет
- Affective DisorderДокумент25 страницAffective DisordermengakuОценок пока нет
- Adhd KasyДокумент11 страницAdhd KasymengakuОценок пока нет
- Attention Deficit and Hyperactivity DisorderДокумент11 страницAttention Deficit and Hyperactivity DisordermengakuОценок пока нет
- The Scopes TrialДокумент10 страницThe Scopes Trialapi-607238202Оценок пока нет
- Final Exam1-Afternoon SessionДокумент40 страницFinal Exam1-Afternoon SessionJoshua Wright0% (1)
- Electrical Information: Service Training MechanikДокумент22 страницыElectrical Information: Service Training Mechanikfroilan ochoaОценок пока нет
- The Divine Liturgy Syro Malankara ChurchДокумент4 страницыThe Divine Liturgy Syro Malankara ChurchGian Marco TallutoОценок пока нет
- NIA Foundation PLI Proposal Template (Repaired)Документ23 страницыNIA Foundation PLI Proposal Template (Repaired)lama dasuОценок пока нет
- Research Design1 USED 6Документ14 страницResearch Design1 USED 6Joselle RuizОценок пока нет
- Meralco v. CastilloДокумент2 страницыMeralco v. CastilloJoven CamusОценок пока нет
- N Advocates Act 1961 Ankita218074 Nujsedu 20221008 230429 1 107Документ107 страницN Advocates Act 1961 Ankita218074 Nujsedu 20221008 230429 1 107ANKITA BISWASОценок пока нет
- Selvanathan-7e 17Документ92 страницыSelvanathan-7e 17Linh ChiОценок пока нет
- Business Finance Chapter 4Документ15 страницBusiness Finance Chapter 4chloe frostОценок пока нет
- Mcqmate Com Topic 333 Fundamentals of Ethics Set 1Документ34 страницыMcqmate Com Topic 333 Fundamentals of Ethics Set 1Veena DeviОценок пока нет
- DocumentДокумент4 страницыDocumentJuliana ZamorasОценок пока нет
- BangaloreДокумент1 229 страницBangaloreVikas RanjanОценок пока нет
- MarshallingДокумент7 страницMarshallinggeetika singhОценок пока нет
- AVERY, Adoratio PurpuraeДокумент16 страницAVERY, Adoratio PurpuraeDejan MitreaОценок пока нет
- Approaching Checklist Final PDFДокумент15 страницApproaching Checklist Final PDFCohort Partnerships100% (1)
- HDLSS Numerical Assignments - DOC FormatДокумент3 страницыHDLSS Numerical Assignments - DOC FormatNikhil UpadhyayОценок пока нет
- The Effectiveness of Peppermint Oil (Mentha X Pepipirita) As Mosquito RepellentДокумент4 страницыThe Effectiveness of Peppermint Oil (Mentha X Pepipirita) As Mosquito RepellentKester PlaydaОценок пока нет
- Victorian AOD Intake Tool Turning Point AuditДокумент8 страницVictorian AOD Intake Tool Turning Point AuditHarjotBrarОценок пока нет
- Sampling Strategies For Heterogeneous WastesДокумент18 страницSampling Strategies For Heterogeneous Wastesmohammed karasnehОценок пока нет
- Firewatch in The History of Walking SimsДокумент5 страницFirewatch in The History of Walking SimsZarahbeth Claire G. ArcederaОценок пока нет
- Position Paper On Sexual Orientation, Gender Identity and Expression (SOGIE)Документ3 страницыPosition Paper On Sexual Orientation, Gender Identity and Expression (SOGIE)SYDNEY MARASIGANОценок пока нет
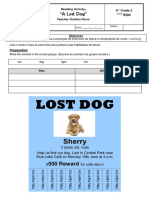
- Reading Activity - A Lost DogДокумент3 страницыReading Activity - A Lost DogGigsFloripaОценок пока нет
- Extreme Risk FinanceДокумент322 страницыExtreme Risk FinanceThomas Thomas100% (2)
- Share Cognitive Notes Doc-1Документ15 страницShare Cognitive Notes Doc-1GinniОценок пока нет
- Chapter 4 - Transfer FunctionsДокумент36 страницChapter 4 - Transfer FunctionsFakhrulShahrilEzanie100% (1)
- Brenda Alderman v. The Philadelphia Housing Authority, 496 F.2d 164, 3rd Cir. (1974)Документ16 страницBrenda Alderman v. The Philadelphia Housing Authority, 496 F.2d 164, 3rd Cir. (1974)Scribd Government DocsОценок пока нет
- Hindu Dharma Parichayam - Swami Parameswarananda SaraswatiДокумент376 страницHindu Dharma Parichayam - Swami Parameswarananda SaraswatiSudarsana Kumar VadasserikkaraОценок пока нет