Вам также может понравиться
- Healing Prayer by Dr. Cindy TrimmДокумент10 страницHealing Prayer by Dr. Cindy TrimmLETHE TATGE93% (27)
- Philhealth Claim Form 4Документ2 страницыPhilhealth Claim Form 4Rolly Rodriguez60% (5)
- Special Operations Forces Medical HandbookОт EverandSpecial Operations Forces Medical HandbookРейтинг: 4.5 из 5 звезд4.5/5 (2)
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtОт EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtРейтинг: 5 из 5 звезд5/5 (1)
- ARDS PPT SlideshareДокумент49 страницARDS PPT Slidesharesonam yadav67% (3)
- ATI - Adult Medical Surgical NGN B (99 Questions and Answers 2023 - Guarantee A+Документ28 страницATI - Adult Medical Surgical NGN B (99 Questions and Answers 2023 - Guarantee A+denis100% (1)
- Respiratory Failure: by ArДокумент39 страницRespiratory Failure: by ArAleksei RomahovОценок пока нет
- DR Muhammed AslamДокумент56 страницDR Muhammed AslamSef NengkoОценок пока нет
- Acute Respiratory Distress Syndrome (Ards) and Sepsis: Frans Abednego Barus Spesialis ParuДокумент29 страницAcute Respiratory Distress Syndrome (Ards) and Sepsis: Frans Abednego Barus Spesialis Paruarif qadhafyОценок пока нет
- ARDS (Handout)Документ3 страницыARDS (Handout)Chin ChinОценок пока нет
- Respiratory FailureДокумент21 страницаRespiratory FailureDennis MiritiОценок пока нет
- Fat Embolism SyndromeДокумент19 страницFat Embolism SyndromeFaizah AlmuhsinОценок пока нет
- Acute Respiratory Distress SyndromДокумент19 страницAcute Respiratory Distress SyndromTaqdees ManzoorОценок пока нет
- Acute Respiratory Distress SyndromeДокумент18 страницAcute Respiratory Distress SyndromeJerinОценок пока нет
- Acute Respiratory Distress SyndromeДокумент17 страницAcute Respiratory Distress SyndromeSherree Hayes100% (2)
- ACUTE RESPIRATORY DISTRESS SYNDROME by Dr. Monday ZaccheausДокумент59 страницACUTE RESPIRATORY DISTRESS SYNDROME by Dr. Monday ZaccheausDr. Amb. Monday ZaccheausОценок пока нет
- Acute Respiratory Distress SyndromeДокумент36 страницAcute Respiratory Distress Syndromedr9348345000Оценок пока нет
- 4th Problem KGD DanielДокумент130 страниц4th Problem KGD DanielSelly HerliaОценок пока нет
- Alka.S.Kandula Roll No: 6Документ15 страницAlka.S.Kandula Roll No: 6Raksha G GowdaОценок пока нет
- Respirotary MnemonicsДокумент9 страницRespirotary MnemonicsAymen Omer0% (1)
- Respiratory FailureДокумент39 страницRespiratory FailureMuntasir BashirОценок пока нет
- Tuti Herawati, MN: Fakultas Ilmu Keperawatan Universitas Indonesia 2008Документ40 страницTuti Herawati, MN: Fakultas Ilmu Keperawatan Universitas Indonesia 2008SelvyaОценок пока нет
- 04 - Pathology of Pulmonary Vascular Diseases 01 - 09 - 2015Документ32 страницы04 - Pathology of Pulmonary Vascular Diseases 01 - 09 - 2015Frederick ChuОценок пока нет
- Acute Respiratory Distress SyndromeДокумент24 страницыAcute Respiratory Distress SyndromePooja ShashidharanОценок пока нет
- ARDSДокумент23 страницыARDSDumora FatmaОценок пока нет
- ARFДокумент50 страницARFAme MehadiОценок пока нет
- Pulmonary EmbolismДокумент96 страницPulmonary Embolismsamice5100% (1)
- Acute Respiratory Distress SyndromeДокумент18 страницAcute Respiratory Distress SyndromeIrham TahkikОценок пока нет
- Dr. K. V. Raman, Dean, MtpgrihsДокумент66 страницDr. K. V. Raman, Dean, MtpgrihsShruti100% (1)
- Acute Respiratory Distress SyndromeДокумент15 страницAcute Respiratory Distress Syndromeamitkulkarni83Оценок пока нет
- Management of Patients With Acute Respiratory Distress SyndromeДокумент41 страницаManagement of Patients With Acute Respiratory Distress Syndrome8515944Оценок пока нет
- Group 1 6 Problem Emergency Medicine Block Monday, 30 Oct 2017Документ121 страницаGroup 1 6 Problem Emergency Medicine Block Monday, 30 Oct 2017Jonathan TandajuОценок пока нет
- By S F Hashmi Guided by DR D G Mhaisekar Sir 22TH FEB 2011Документ57 страницBy S F Hashmi Guided by DR D G Mhaisekar Sir 22TH FEB 2011Fazlullah Hashmi100% (1)
- ARDS (Acute Respiratory Distress Syndrome)Документ38 страницARDS (Acute Respiratory Distress Syndrome)Zahrine HananiОценок пока нет
- Acute Respiratory Distress Syndrome (Ards) : Muamar Aldalaeen, RN, Mba, HCRM, Cic, Ipm, MSN, Phd. Haneen Alnuaimi, MSNДокумент59 страницAcute Respiratory Distress Syndrome (Ards) : Muamar Aldalaeen, RN, Mba, HCRM, Cic, Ipm, MSN, Phd. Haneen Alnuaimi, MSNAboodsha ShОценок пока нет
- Acute Respiratory Distress SyndromeДокумент9 страницAcute Respiratory Distress Syndromerania salsabilaОценок пока нет
- Pulmonary Edema: - by Fitsum Solomon Fireneh Niguse G/Michael G/Meskel Gemechisa DaluДокумент57 страницPulmonary Edema: - by Fitsum Solomon Fireneh Niguse G/Michael G/Meskel Gemechisa DaluashuОценок пока нет
- Acute Respiratory Distress SyndromeДокумент18 страницAcute Respiratory Distress SyndromeNitnotGundilОценок пока нет
- Ards PDFДокумент73 страницыArds PDFdr.Nugroho PrasetyoОценок пока нет
- Approach To Common Respiratory DiseaseДокумент57 страницApproach To Common Respiratory DiseaseRajhmuniran KandasamyОценок пока нет
- Edema ParuДокумент28 страницEdema ParuSantiFaridKalukuОценок пока нет
- 4-1pulmonary DisordersДокумент38 страниц4-1pulmonary DisordersAbdallah AlasalОценок пока нет
- Chronic Obstructive Pulmonary Disease: TH NDДокумент22 страницыChronic Obstructive Pulmonary Disease: TH NDSuhaila Naif NasserОценок пока нет
- Acute Respiratory Distress Syndrome (Ards)Документ14 страницAcute Respiratory Distress Syndrome (Ards)salma wangie fОценок пока нет
- ARDSДокумент12 страницARDSMarius Clifford BilledoОценок пока нет
- Senior Talk - ARDSДокумент44 страницыSenior Talk - ARDSDrMohammed FouaadОценок пока нет
- Pulmonary Edema: Dr. Harsh Pandya R1 Under Guidance of DR - Nipa Nayak M.D. Asso. ProfДокумент49 страницPulmonary Edema: Dr. Harsh Pandya R1 Under Guidance of DR - Nipa Nayak M.D. Asso. ProfKrisno ParammanganОценок пока нет
- Atelectasis: CausesДокумент4 страницыAtelectasis: Causesaznknight323Оценок пока нет
- Diagnosis: ARDS OverviewДокумент5 страницDiagnosis: ARDS OverviewLuvita RonteltapОценок пока нет
- Trali, Taco and TadДокумент45 страницTrali, Taco and Taddr AmitОценок пока нет
- ArdsДокумент48 страницArdsvmalik985Оценок пока нет
- Syok SepticДокумент15 страницSyok SepticJennifer GraceОценок пока нет
- Acute Pulmonary Edema: Purwoko Sugeng HДокумент25 страницAcute Pulmonary Edema: Purwoko Sugeng HBee DanielОценок пока нет
- Acute Respiratory Distress Syndrome: Dewi Kartikawati NДокумент29 страницAcute Respiratory Distress Syndrome: Dewi Kartikawati NAnonymous 0Mnt71Оценок пока нет
- Hypoxemia in ICU: Prepared by Hadi JazanДокумент41 страницаHypoxemia in ICU: Prepared by Hadi JazanHadi JazanОценок пока нет
- 01.practic QuestionsДокумент12 страниц01.practic QuestionsEdu Deea CazacuОценок пока нет
- Running A Race at 12,000 FeetДокумент39 страницRunning A Race at 12,000 FeetAndela Ernesto HenriqueОценок пока нет
- Pemicu 6 KGD AldiДокумент134 страницыPemicu 6 KGD AldiFirdaus AldyОценок пока нет
- Acute Respiratory Distress Syndrome (ARDS) : Dewa Artika Devisi Paru / Lab - Ip.Dalam FK Unud - Rsup SanglahДокумент26 страницAcute Respiratory Distress Syndrome (ARDS) : Dewa Artika Devisi Paru / Lab - Ip.Dalam FK Unud - Rsup SanglahKessi VikaneswariОценок пока нет
- Acute Respiratory FailureДокумент17 страницAcute Respiratory FailurejulianajosОценок пока нет
- Respiratory Failure: Dr. Sat Sharma Univ of ManitobaДокумент38 страницRespiratory Failure: Dr. Sat Sharma Univ of ManitobaGonzalo Venegas RojasОценок пока нет
- Lung Diseases Lydia Tantoso, MD, INTERNISTДокумент28 страницLung Diseases Lydia Tantoso, MD, INTERNISTgrace liwantoОценок пока нет
- Suicide Risk Evaluation: Case Presentation and Clinical DiscussionДокумент52 страницыSuicide Risk Evaluation: Case Presentation and Clinical DiscussionRoya FarooqОценок пока нет
- Economics AnnualДокумент13 страницEconomics AnnualnamlaskhanОценок пока нет
- Intermediate AccountingДокумент44 страницыIntermediate AccountingRoya FarooqОценок пока нет
- Economic and Social Development App 2014 - 15Документ4 страницыEconomic and Social Development App 2014 - 15Roya FarooqОценок пока нет
- CV Template Classic WorkДокумент2 страницыCV Template Classic WorkRoya FarooqОценок пока нет
- Working Capital ManagementДокумент11 страницWorking Capital ManagementRoya FarooqОценок пока нет
- ALiEM in Training Exam Review Book HyperlinkedДокумент388 страницALiEM in Training Exam Review Book HyperlinkedcalstudyОценок пока нет
- Heart FailureДокумент108 страницHeart FailureDeasy Rizka Rahmawati100% (1)
- Chest Pain Case Write-Up - Doctoring IIIДокумент4 страницыChest Pain Case Write-Up - Doctoring IIIchristietwongОценок пока нет
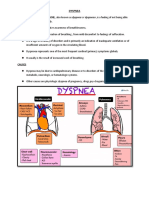
- Dyspnea: CausesДокумент7 страницDyspnea: CausesGetom NgukirОценок пока нет
- CardiomyopathyДокумент18 страницCardiomyopathyDimpal Choudhary100% (1)
- Bates Thorax Lungs With TermsДокумент4 страницыBates Thorax Lungs With Termscrystalshe100% (1)
- Respiratory System Muamar Aldalaeen, RN, Mba, HCRM, Cic, Ipm, MSN, PHD - Haneen Alnuaimi, MSNДокумент46 страницRespiratory System Muamar Aldalaeen, RN, Mba, HCRM, Cic, Ipm, MSN, PHD - Haneen Alnuaimi, MSNAboodsha ShОценок пока нет
- Zanki Respiratory PathologyДокумент15 страницZanki Respiratory Pathologysmian08100% (1)
- Respiratory Status of Adult Patients in The Postoperative Period of Thoracic or Upper Abdominal SurgeriesДокумент8 страницRespiratory Status of Adult Patients in The Postoperative Period of Thoracic or Upper Abdominal SurgeriesDimitreОценок пока нет
- Medical Assessment Station 3BДокумент2 страницыMedical Assessment Station 3BGriffin PОценок пока нет
- Study of Efficacy of Active Cycle of Breathing TechniquesДокумент89 страницStudy of Efficacy of Active Cycle of Breathing Techniquesnaga9390051055Оценок пока нет
- REVISED Group4 Congestive Heart FailureДокумент64 страницыREVISED Group4 Congestive Heart FailureNicole Villanueva, BSN - Level 3AОценок пока нет
- Case Scenarios University DR - NerveДокумент24 страницыCase Scenarios University DR - NerveSREE NITHINОценок пока нет
- How To Take HistoryДокумент59 страницHow To Take HistoryBelalОценок пока нет
- Physiotherapy Guideline: Queensland Cardiorespiratory Physiotherapy NetworkДокумент20 страницPhysiotherapy Guideline: Queensland Cardiorespiratory Physiotherapy NetworkBRDОценок пока нет
- SERETIDEДокумент3 страницыSERETIDETempoОценок пока нет
- Etiologic FactorsДокумент1 страницаEtiologic FactorsMARIA CHARMIN M. MEJIAОценок пока нет
- Penatalaksanaan Petugas Terpapar COVID-19Документ30 страницPenatalaksanaan Petugas Terpapar COVID-19Taupick ArsyОценок пока нет
- Block Q IM Orals ReviewerДокумент107 страницBlock Q IM Orals ReviewerCarl Vin PasionОценок пока нет
- NCP CKD From CaneДокумент74 страницыNCP CKD From CaneSheela Khrystyn LeeОценок пока нет
- OET Al-Ghazouly Writing Final-RevisionДокумент38 страницOET Al-Ghazouly Writing Final-Revisiondr.aliceОценок пока нет
- Specific Types of DysnpeaДокумент14 страницSpecific Types of DysnpeaPiyush Agarwal100% (1)
- Acute Respiratory FailureДокумент2 страницыAcute Respiratory FailureCharis ParoginogОценок пока нет
- Internal Medicine HEARTДокумент10 страницInternal Medicine HEARTpeter911xОценок пока нет
- Mnemonics On Pathology and MicrobiologyДокумент105 страницMnemonics On Pathology and MicrobiologyJessica Advíncula100% (1)
- Lived Experiences Wiith Covid - 19Документ9 страницLived Experiences Wiith Covid - 19Freddy JunsayОценок пока нет
- EuroHeart Failure Survey II A Survey On Hospitalized Acute Heart Failure PatientsДокумент12 страницEuroHeart Failure Survey II A Survey On Hospitalized Acute Heart Failure PatientsEffika PutriОценок пока нет