Вам также может понравиться
- Anti-Hbs (Hepatitis B Immune Status/Anti-Hepatitis B Surface Antibody)Документ3 страницыAnti-Hbs (Hepatitis B Immune Status/Anti-Hepatitis B Surface Antibody)rocker_jadulОценок пока нет
- Opportunistic InfectionsДокумент88 страницOpportunistic InfectionszamadulaОценок пока нет
- Hep B Request FormДокумент1 страницаHep B Request FormMuaz AbdullahОценок пока нет
- Graft Vs Host DiseaseДокумент44 страницыGraft Vs Host DiseaseHasna Mirda AmazanОценок пока нет
- Acute Cholecystitis and The Timing of Surgery:: When Is It Time To Heal With Steel?Документ48 страницAcute Cholecystitis and The Timing of Surgery:: When Is It Time To Heal With Steel?Ahmad MullaОценок пока нет
- General Surgery SMALL INTESTINES-Dr MendozaДокумент101 страницаGeneral Surgery SMALL INTESTINES-Dr MendozaMedisina101Оценок пока нет
- β-Lactam Antibiotics: carbapenemsДокумент14 страницβ-Lactam Antibiotics: carbapenemsim. EliasОценок пока нет
- Interpretation of CBCДокумент35 страницInterpretation of CBCnth1992Оценок пока нет
- Surgical Diseases of The EsophagusДокумент35 страницSurgical Diseases of The Esophagusmogesie1995Оценок пока нет
- Typhoid Ileal Perforation: DR - ArifusmanДокумент28 страницTyphoid Ileal Perforation: DR - ArifusmanMudassar SaeedОценок пока нет
- Abg Interpretation: Sidra Yousaf, RNДокумент37 страницAbg Interpretation: Sidra Yousaf, RNIhtesham Ul HaqОценок пока нет
- Lecture: Adrenal DisordersДокумент78 страницLecture: Adrenal DisordersOchendo KingxОценок пока нет
- Chest IntubationДокумент42 страницыChest IntubationdrusmanjamilhcmdОценок пока нет
- Upper Gi BleedДокумент20 страницUpper Gi BleedNaeem Shehzad100% (1)
- Hypertension and Angina DrugsДокумент158 страницHypertension and Angina DrugsMelissa SalayogОценок пока нет
- Grafts-Flaps and Tissue TransplantationДокумент68 страницGrafts-Flaps and Tissue Transplantationdaniel situngkir100% (1)
- Pepti C Ul Cer Dis Ea SeДокумент36 страницPepti C Ul Cer Dis Ea Segerald_ichigoОценок пока нет
- Surgical Disease of Spleen Part 2Документ52 страницыSurgical Disease of Spleen Part 2Rashed ShatnawiОценок пока нет
- The Spleen - A Surgical Perspective: by Col. Abrar Hussain ZaidiДокумент43 страницыThe Spleen - A Surgical Perspective: by Col. Abrar Hussain Zaidiabrar_zaidiОценок пока нет
- Non Viral HepatitisДокумент40 страницNon Viral Hepatitisostaz2000100% (1)
- The Pharyngeal Apparatus: - Face, Nasal Cavities, MouthДокумент73 страницыThe Pharyngeal Apparatus: - Face, Nasal Cavities, MouthKhasibatul AuliaОценок пока нет
- Genital Surgical DiseasesДокумент18 страницGenital Surgical DiseasesanojОценок пока нет
- Acute Abdomen &peritonitisДокумент63 страницыAcute Abdomen &peritonitisSamar Ahmad100% (1)
- Drug-Induced QT Interval ProlongationДокумент13 страницDrug-Induced QT Interval ProlongationgeoaislaОценок пока нет
- Tumour Marker For Medincine ResidentsДокумент58 страницTumour Marker For Medincine ResidentsSandeep NarayananОценок пока нет
- Peptic Ulcer DiseaseДокумент14 страницPeptic Ulcer DiseasePernel Jose Alam MicuboОценок пока нет
- Biliary Tract Cancer: Presented By: DR Ankit Lalchandani Moderated By: DR MP SinghДокумент36 страницBiliary Tract Cancer: Presented By: DR Ankit Lalchandani Moderated By: DR MP SinghAnkit LalchandaniОценок пока нет
- Breast CancerДокумент6 страницBreast Cancersarguss14Оценок пока нет
- Shock (For Surgery)Документ50 страницShock (For Surgery)Emmanuel Rojith VazОценок пока нет
- 13Lec-Approach To Neonates With Suspected Congenital InfectionsДокумент56 страниц13Lec-Approach To Neonates With Suspected Congenital InfectionsMinerva Stanciu100% (1)
- 1.rationale of Use of Antibiotic in Surgical Patients CДокумент22 страницы1.rationale of Use of Antibiotic in Surgical Patients CPanna SahaОценок пока нет
- Pyloric StenosisДокумент23 страницыPyloric StenosisRama ItachiОценок пока нет
- Emergency DrugsДокумент10 страницEmergency DrugsnieacatleyaОценок пока нет
- 1 Hepatic NeoplasmsДокумент19 страниц1 Hepatic NeoplasmsAldino Siwa PutraОценок пока нет
- TB in Children: Department of Pediatrics College of Medicine Cagayan State UniversityДокумент49 страницTB in Children: Department of Pediatrics College of Medicine Cagayan State UniversityyayayanizaОценок пока нет
- Overview of HIV and Its Management: Caroline Mills-Davies Emmanuel FantevieДокумент101 страницаOverview of HIV and Its Management: Caroline Mills-Davies Emmanuel FantevieImanuel Fantevie100% (1)
- How To Read A CTGДокумент31 страницаHow To Read A CTGAbdullah As'ad100% (1)
- Gallbladder EmpyemaДокумент17 страницGallbladder EmpyemaYayut 18Оценок пока нет
- Viral CarcinogenesisДокумент18 страницViral CarcinogenesisTowardsLightОценок пока нет
- Evaluation of Liver FunctionДокумент64 страницыEvaluation of Liver FunctionMustafa KhandgawiОценок пока нет
- Pediatric Department Faculty of MedicineДокумент100 страницPediatric Department Faculty of MedicineIrfanОценок пока нет
- Pathogens of The Female Reproductive System - Leah NechamkinДокумент1 страницаPathogens of The Female Reproductive System - Leah NechamkinMicroposterОценок пока нет
- City of Batac, Ilocos Norte, Philippines Contact Details: Direct Line: (077) 6000105 Trunk Line: (077) 7923133 Loc. 102Документ1 страницаCity of Batac, Ilocos Norte, Philippines Contact Details: Direct Line: (077) 6000105 Trunk Line: (077) 7923133 Loc. 102LexiePascuaSantosОценок пока нет
- Chronic Leukemia: Rahmawati Minhajat A. Fachruddin BenyaminДокумент24 страницыChronic Leukemia: Rahmawati Minhajat A. Fachruddin BenyaminMJ Putra100% (1)
- Ssat Absite Review: HPB: Douglas Cassidy, MD MGH Surgical Education Research and Simulation FellowДокумент19 страницSsat Absite Review: HPB: Douglas Cassidy, MD MGH Surgical Education Research and Simulation FellowmikhailОценок пока нет
- Beta LactamДокумент2 страницыBeta LactamJayde TabanaoОценок пока нет
- Pancreatic AdenocarcinomaДокумент6 страницPancreatic AdenocarcinomafikriafisОценок пока нет
- Thyroidectomy Morbidities:: Preventions & InterventionsДокумент52 страницыThyroidectomy Morbidities:: Preventions & InterventionsAlfonso DanacОценок пока нет
- Clinical Management: PGI Eileen Andres PediatricsДокумент9 страницClinical Management: PGI Eileen Andres PediatricsMichael BonillaОценок пока нет
- Polycystic Kidney DiseaseДокумент9 страницPolycystic Kidney DiseaseCésar Aguilar ContrerasОценок пока нет
- Perforated Peptic UlcerДокумент68 страницPerforated Peptic UlcerSaibo BoldsaikhanОценок пока нет
- Peptic Ulcer Disease: Dr. Haji Bahadar Pharmd, PHD Assistant Professor Khyber Medical University-PeshawarДокумент24 страницыPeptic Ulcer Disease: Dr. Haji Bahadar Pharmd, PHD Assistant Professor Khyber Medical University-Peshawarms khan100% (1)
- CC C C: June 8, 2011 By: Santos, Edilberto DBДокумент63 страницыCC C C: June 8, 2011 By: Santos, Edilberto DBHakugeiОценок пока нет
- Ascitic Fluid AnalysisДокумент3 страницыAscitic Fluid AnalysisLohJОценок пока нет
- Pathology Bleeding DisordersДокумент67 страницPathology Bleeding DisordersMarcelliaОценок пока нет
- Palliative EnciesДокумент96 страницPalliative EnciesnandanОценок пока нет
- Acute Abdomen: - DefinitionДокумент27 страницAcute Abdomen: - DefinitionWorku KifleОценок пока нет
- Systemic Lupus Erythematosus Lecture Salah Abdel BakyДокумент8 страницSystemic Lupus Erythematosus Lecture Salah Abdel Bakyahmed gabrОценок пока нет
- Evaluation of Abdominal PainДокумент7 страницEvaluation of Abdominal PainCherry Faith Merisco LabtangОценок пока нет
- Bahan KKD KeputihanДокумент26 страницBahan KKD KeputihanangelinaОценок пока нет
- Alimentatia Copilului - OMSДокумент112 страницAlimentatia Copilului - OMSshugyosha77Оценок пока нет
- Ujian AnakДокумент122 страницыUjian AnakangelinaОценок пока нет
- Battisti Nnconvulsions enДокумент130 страницBattisti Nnconvulsions enangelinaОценок пока нет
- Scrib TenДокумент4 страницыScrib TenangelinaОценок пока нет
- Battisti Nnconvulsions enДокумент130 страницBattisti Nnconvulsions enangelinaОценок пока нет
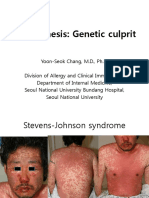
- Toxic Epidermal NecrolysisДокумент23 страницыToxic Epidermal NecrolysisangelinaОценок пока нет
- Sladden Et Al 2005 enДокумент13 страницSladden Et Al 2005 enangelinaОценок пока нет
- 27 PPTДокумент47 страниц27 PPTangelinaОценок пока нет
- Charlie Pemicu 4 EtikaДокумент34 страницыCharlie Pemicu 4 EtikaangelinaОценок пока нет
- TenДокумент10 страницTenangelinaОценок пока нет
- Guide Neonate WHO PDFДокумент100 страницGuide Neonate WHO PDFSherlocknov100% (1)
- InhibitorДокумент21 страницаInhibitorAnonymous 1gH7ra9AОценок пока нет
- Prodromal - Aura - Nyeri Kepala - PostdormalДокумент15 страницProdromal - Aura - Nyeri Kepala - PostdormalangelinaОценок пока нет
- Biokimia - Heme DegradationДокумент17 страницBiokimia - Heme DegradationangelinaОценок пока нет
- Pemicu 4 Uro RifkieДокумент94 страницыPemicu 4 Uro RifkieangelinaОценок пока нет
- Report A Case of Perinatal Hepatitis BДокумент2 страницыReport A Case of Perinatal Hepatitis BangelinaОценок пока нет
- ACS Therapy Algorithm WEB SecureДокумент1 страницаACS Therapy Algorithm WEB SecureAmelia Cassandra ChatabОценок пока нет
- 27 PPTДокумент47 страниц27 PPTangelinaОценок пока нет
- VIRUSESДокумент21 страницаVIRUSESSome BodyОценок пока нет
- The JKL Medical DictionaryДокумент186 страницThe JKL Medical Dictionarymoekyaw7171Оценок пока нет
- Exam Questions For Microboilogy, Virology 2022-2023Документ10 страницExam Questions For Microboilogy, Virology 2022-2023Amirus RussОценок пока нет
- Animal BiotechДокумент13 страницAnimal BiotechAjay Pratap Singh Chauhan100% (1)
- Covid Reference 04Документ376 страницCovid Reference 04Federico Soldani100% (1)
- Antivirales Orales de Primera Generación Contra El SARS CoV 2 ClinicalДокумент21 страницаAntivirales Orales de Primera Generación Contra El SARS CoV 2 ClinicalCarmenОценок пока нет
- Unveiling The Covid19 Pandemic Research 2021Документ33 страницыUnveiling The Covid19 Pandemic Research 2021Anmesh keru100% (1)
- Ozone Therapy: A Clinical ReviewДокумент5 страницOzone Therapy: A Clinical ReviewSteveОценок пока нет
- Public Health: Inside Listening and Speaking 3 Unit 4 Answer KeyДокумент4 страницыPublic Health: Inside Listening and Speaking 3 Unit 4 Answer KeyLâm Duy67% (3)
- Nakita Harris - VIRUS READING (LYTIC & LYSOGENIC)Документ2 страницыNakita Harris - VIRUS READING (LYTIC & LYSOGENIC)Nakita HarrisОценок пока нет
- Essay On Corporate CultureДокумент6 страницEssay On Corporate CultureezmsdedpОценок пока нет
- Comprehensive Revision Test - Basics 1Документ16 страницComprehensive Revision Test - Basics 1drpnnreddyОценок пока нет
- Benefit of Covid-19 VaccineДокумент9 страницBenefit of Covid-19 VaccineKevo KarisОценок пока нет
- Agglutination ReactionsДокумент28 страницAgglutination Reactionsstevie watuna100% (1)
- Biology Asoe 2015 Part A BДокумент28 страницBiology Asoe 2015 Part A BАрхи́пОценок пока нет
- Https /app - Ieltsninja.com/quiz Test/5/336631/ Method PaperДокумент11 страницHttps /app - Ieltsninja.com/quiz Test/5/336631/ Method PaperBALKRISHNAОценок пока нет
- Microbial Detection Total Solution: MGI Sequencing Platform For Pathogen Fast IdentificationДокумент20 страницMicrobial Detection Total Solution: MGI Sequencing Platform For Pathogen Fast IdentificationEntio BaezОценок пока нет
- Animal HusbandryДокумент21 страницаAnimal HusbandryKshiteeja DushingОценок пока нет
- HepatitisДокумент11 страницHepatitistorsedepointeОценок пока нет
- MyocarditisДокумент29 страницMyocarditispanvilai0% (1)
- CH 43 ImmunityДокумент71 страницаCH 43 ImmunityNaveen Kishore GattimОценок пока нет
- BOOK Gene TherapyДокумент210 страницBOOK Gene TherapyCarla GomesОценок пока нет
- Goljan RR - ImmunopathologyДокумент13 страницGoljan RR - ImmunopathologyShaz ChindhyОценок пока нет
- AQA GCSE Bio End of Topic B6Документ8 страницAQA GCSE Bio End of Topic B6John HoltОценок пока нет
- ScabiesДокумент16 страницScabiescarla_sarmiento4847Оценок пока нет
- Diseases With The Rash Syndrome11.Документ33 страницыDiseases With The Rash Syndrome11.ManishОценок пока нет
- Gen Bio Mock QuizДокумент6 страницGen Bio Mock QuizJarvis RazonОценок пока нет
- BIOLOGYДокумент255 страницBIOLOGYC InsightОценок пока нет
- Agriculture Junior Secondary School (Jss 2) First TermДокумент4 страницыAgriculture Junior Secondary School (Jss 2) First TermErnest Belamo100% (1)
- The Covid-19 Pandemic and Haemoglobin Disorders: Vaccinations & Therapeutic DrugsДокумент53 страницыThe Covid-19 Pandemic and Haemoglobin Disorders: Vaccinations & Therapeutic DrugsJuanGabrielVillamizarОценок пока нет
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicОт EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicОценок пока нет
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisОт EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisРейтинг: 4 из 5 звезд4/5 (9)
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineОт EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineОценок пока нет
- The Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthОт EverandThe Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthОценок пока нет
- Summary: The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health by Robert F. Kennedy Jr: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health by Robert F. Kennedy Jr: Key Takeaways, Summary & Analysis IncludedОценок пока нет
- Inflamed: Deep Medicine and the Anatomy of InjusticeОт EverandInflamed: Deep Medicine and the Anatomy of InjusticeРейтинг: 5 из 5 звезд5/5 (12)
- The Bodies of Others: The New Authoritarians, COVID-19 and The War Against the HumanОт EverandThe Bodies of Others: The New Authoritarians, COVID-19 and The War Against the HumanРейтинг: 4.5 из 5 звезд4.5/5 (12)
- Epic Measures: One Doctor. Seven Billion Patients.От EverandEpic Measures: One Doctor. Seven Billion Patients.Рейтинг: 4 из 5 звезд4/5 (13)
- There Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceОт EverandThere Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceРейтинг: 4.5 из 5 звезд4.5/5 (11)
- There Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceОт EverandThere Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceРейтинг: 4.5 из 5 звезд4.5/5 (15)
- The Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsОт EverandThe Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsРейтинг: 4.5 из 5 звезд4.5/5 (6)
- Mama Might Be Better Off Dead: The Failure of Health Care in Urban AmericaОт EverandMama Might Be Better Off Dead: The Failure of Health Care in Urban AmericaОценок пока нет
- Fatal Conveniences: The Toxic Products and Harmful Habits That Are Making You Sick—and the Simple Changes That Will Save Your HealthОт EverandFatal Conveniences: The Toxic Products and Harmful Habits That Are Making You Sick—and the Simple Changes That Will Save Your HealthРейтинг: 4 из 5 звезд4/5 (7)
- Clean: Overcoming Addiction and Ending America’s Greatest TragedyОт EverandClean: Overcoming Addiction and Ending America’s Greatest TragedyРейтинг: 4 из 5 звезд4/5 (18)
- Vaccines Did Not Cause Rachel's Autism: My Journey as a Vaccine Scientist, Pediatrician, and Autism DadОт EverandVaccines Did Not Cause Rachel's Autism: My Journey as a Vaccine Scientist, Pediatrician, and Autism DadРейтинг: 4.5 из 5 звезд4.5/5 (3)
- The Wuhan Cover-Up: And the Terrifying Bioweapons Arms RaceОт EverandThe Wuhan Cover-Up: And the Terrifying Bioweapons Arms RaceОценок пока нет
- Heat Wave: A Social Autopsy of Disaster in ChicagoОт EverandHeat Wave: A Social Autopsy of Disaster in ChicagoРейтинг: 4 из 5 звезд4/5 (40)
- The Inescapable Immune Escape PandemicОт EverandThe Inescapable Immune Escape PandemicРейтинг: 5 из 5 звезд5/5 (1)
- Breaking out of the Health Care Abyss: Transformational Tips for Agents of ChangeОт EverandBreaking out of the Health Care Abyss: Transformational Tips for Agents of ChangeОценок пока нет
- Beyond the Next Village: A Year of Magic and Medicine in NepalОт EverandBeyond the Next Village: A Year of Magic and Medicine in NepalОценок пока нет
- The Truth about Wuhan: How I Uncovered the Biggest Lie in HistoryОт EverandThe Truth about Wuhan: How I Uncovered the Biggest Lie in HistoryРейтинг: 4 из 5 звезд4/5 (6)
- The Invisible Rainbow: A History of Electricity and LifeОт EverandThe Invisible Rainbow: A History of Electricity and LifeРейтинг: 4.5 из 5 звезд4.5/5 (21)
- COVID-19: The Victims, The Heroes, The Comlicit, and Our New NormalОт EverandCOVID-19: The Victims, The Heroes, The Comlicit, and Our New NormalОценок пока нет
- Healthy Buildings: How Indoor Spaces Drive Performance and ProductivityОт EverandHealthy Buildings: How Indoor Spaces Drive Performance and ProductivityРейтинг: 5 из 5 звезд5/5 (2)