Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- Moderna Vs PfizerДокумент7 страницModerna Vs PfizerAlkausarОценок пока нет
- Adam Goleman Emotionl Inteligence Non Violent ComunicationДокумент655 страницAdam Goleman Emotionl Inteligence Non Violent Comunicationtomy100% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Vsim Isbar Activity Student Worksheet: Your Name, Position (RN), Unit You Are Working OnДокумент2 страницыVsim Isbar Activity Student Worksheet: Your Name, Position (RN), Unit You Are Working OnA PОценок пока нет
- WHO TootlkitДокумент88 страницWHO TootlkitVivek BasnetОценок пока нет
- Risk Analysis Power PointДокумент22 страницыRisk Analysis Power PointjupmulОценок пока нет
- Lipton Ice Tea Final Report1Документ113 страницLipton Ice Tea Final Report1Lochana Madushanka75% (4)
- A Complete Guide To The Secrets of Sexual Transmutation: Usp SharingДокумент12 страницA Complete Guide To The Secrets of Sexual Transmutation: Usp SharingGeorgia Alessandra Pareñas Cañaveral100% (2)
- Irrigating Solution in Pediatric DentistryДокумент12 страницIrrigating Solution in Pediatric DentistryshireenopalОценок пока нет
- Fundamentals of Nursing Questionnaire With Answer Key (Lippincott Manual of Nursing Practice)Документ6 страницFundamentals of Nursing Questionnaire With Answer Key (Lippincott Manual of Nursing Practice)YujenОценок пока нет
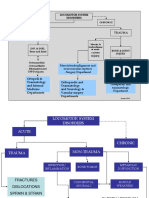
- Introduction of Musculosceletal Disorder and TraumaДокумент19 страницIntroduction of Musculosceletal Disorder and TraumaNdz1Оценок пока нет
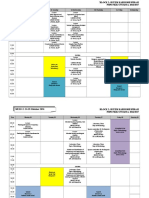
- Jadwal Blok 5 Hema Dan ImunДокумент10 страницJadwal Blok 5 Hema Dan ImunNdz1Оценок пока нет
- Case Report Chrysomya Bezziana: Oral Myiasis Caused by in Anterior MaxillaДокумент5 страницCase Report Chrysomya Bezziana: Oral Myiasis Caused by in Anterior MaxillaNdz1Оценок пока нет
- Citation-51832066 RisДокумент1 страницаCitation-51832066 RisNdz1Оценок пока нет
- Overview Blok 5 Sistem Hematologi Dan ImmunologiДокумент17 страницOverview Blok 5 Sistem Hematologi Dan ImmunologiNdz1Оценок пока нет
- Pengobatan Pasien Tuberkulosis Paru dengan Multidrug Resistant (TB-MDRДокумент13 страницPengobatan Pasien Tuberkulosis Paru dengan Multidrug Resistant (TB-MDRNdz1Оценок пока нет
- Hipotiroid+ Nodul TiroidДокумент61 страницаHipotiroid+ Nodul TiroidPuji AstutiОценок пока нет
- Periorificial Dermatitis in Children An Update and Description of A ChildДокумент3 страницыPeriorificial Dermatitis in Children An Update and Description of A ChildNdz1Оценок пока нет
- Bone and NutritionДокумент36 страницBone and NutritionNdz1Оценок пока нет
- INTOLERANSI LAKTOSAДокумент9 страницINTOLERANSI LAKTOSAmiraОценок пока нет
- Introduction of Musculosceletal Disorder and TraumaДокумент19 страницIntroduction of Musculosceletal Disorder and TraumaNdz1Оценок пока нет
- Revisi Blok 2 Kardioresp-2Документ7 страницRevisi Blok 2 Kardioresp-2Ndz1Оценок пока нет
- Introduction of Musculosceletal Disorder and TraumaДокумент19 страницIntroduction of Musculosceletal Disorder and TraumaNdz1Оценок пока нет
- Menu BazarДокумент3 страницыMenu BazarNdz1Оценок пока нет
- HypertensionДокумент37 страницHypertensionNdz1Оценок пока нет
- Acute Heart Failure: Venice Chairiadi, MD, FIHAДокумент55 страницAcute Heart Failure: Venice Chairiadi, MD, FIHANdz1Оценок пока нет
- 32 63 1 SMДокумент5 страниц32 63 1 SMNdz1Оценок пока нет
- 92 104 April Vol - 30 No - 2 2010 - 2Документ13 страниц92 104 April Vol - 30 No - 2 2010 - 2Paula CyntiaОценок пока нет
- 6334 12340 3 PBДокумент7 страниц6334 12340 3 PBNdz1Оценок пока нет
- 181 355 1 PBДокумент6 страниц181 355 1 PBRezy Arina PutriОценок пока нет
- Bakteri MuskuloskeletalДокумент41 страницаBakteri MuskuloskeletalNdz1Оценок пока нет
- 14 C Neuropsychological Assessment in ChildrenДокумент7 страниц14 C Neuropsychological Assessment in ChildrenSifra Turu AlloОценок пока нет
- 00 CM-HSE-SWP-02 Incident ReportingДокумент5 страниц00 CM-HSE-SWP-02 Incident ReportingTigor GurningОценок пока нет
- Shark Fitness Gym 2.0Документ1 страницаShark Fitness Gym 2.0gourav singhОценок пока нет
- Mission COVID SurakshaДокумент3 страницыMission COVID SurakshaSahilHoodaОценок пока нет
- An Approach To INI-CETДокумент56 страницAn Approach To INI-CETTauseef100% (1)
- NSAT Mathematics and English Scores RelationshipДокумент2 страницыNSAT Mathematics and English Scores RelationshipSoriano AnjelynОценок пока нет
- NRSG 780 - Health Promotion and Population Health: Module 3: EpidemiologyДокумент34 страницыNRSG 780 - Health Promotion and Population Health: Module 3: EpidemiologyjustdoyourОценок пока нет
- Resourse GuideДокумент2 страницыResourse Guideapi-473896951Оценок пока нет
- 11 HUMSS Earth and Life ScienceДокумент1 страница11 HUMSS Earth and Life ScienceAngel Abigail TapayanОценок пока нет
- Management of Neurodermatitis On The Elderly in Kota Karang VillageДокумент6 страницManagement of Neurodermatitis On The Elderly in Kota Karang VillagedewiОценок пока нет
- Science: Brgy. Tampo, Botolan, ZambalesДокумент14 страницScience: Brgy. Tampo, Botolan, ZambalesKeanna Mae DumaplinОценок пока нет
- ANNEX DQAC Member List 29 OctДокумент29 страницANNEX DQAC Member List 29 OctSpace HR100% (1)
- Case - Parkinson's DiseaseДокумент13 страницCase - Parkinson's DiseaseAbin PОценок пока нет
- Nevada CTE Recommended Equipment for Foods and Nutrition ProgramsДокумент2 страницыNevada CTE Recommended Equipment for Foods and Nutrition Programsnithya nithyaОценок пока нет
- Edwin Owwa2 PDFДокумент1 страницаEdwin Owwa2 PDFEdwin AndradaОценок пока нет
- DAFTAR PUSTAKA REFERENCES LISTДокумент3 страницыDAFTAR PUSTAKA REFERENCES LISTBagas SetiawanОценок пока нет
- Workbook 29Документ16 страницWorkbook 29Nerio BrachoОценок пока нет
- 1.principles of Business EthicsДокумент7 страниц1.principles of Business Ethicslegacy guptaОценок пока нет
- Construct Validity of The Relationship Profile Test Links With Attachment, Identity, Relatedness and Affect. Bornstein 2002Документ9 страницConstruct Validity of The Relationship Profile Test Links With Attachment, Identity, Relatedness and Affect. Bornstein 2002Cualit14Оценок пока нет
- Professional Teachers (Secondary) 10-2022 Physical ScienceДокумент13 страницProfessional Teachers (Secondary) 10-2022 Physical SciencePRC BaguioОценок пока нет
- Operation & Service Manual: Model: 18-4208-0010 Four Bottle Nitrogen Cart With Booster and Manifold/RegulatorДокумент49 страницOperation & Service Manual: Model: 18-4208-0010 Four Bottle Nitrogen Cart With Booster and Manifold/Regulatorhb Corp100% (2)