Вам также может понравиться
- Lecture 15 Bowl EliminationДокумент72 страницыLecture 15 Bowl EliminationIsbelОценок пока нет
- BNC Lesson 1-4Документ34 страницыBNC Lesson 1-4Alyssa LoisОценок пока нет
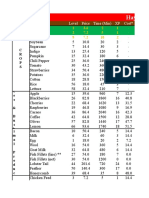
- Hay Day Price Profit AnalysisДокумент112 страницHay Day Price Profit AnalysisCunCunAlAndraОценок пока нет
- Hay Day Price Profit AnalysisДокумент112 страницHay Day Price Profit AnalysisCunCunAlAndraОценок пока нет
- Hay Day Price Profit AnalysisДокумент112 страницHay Day Price Profit AnalysisCunCunAlAndraОценок пока нет
- New Holland Ec25 Mini ExcavatorДокумент153 страницыNew Holland Ec25 Mini ExcavatorJack StinerОценок пока нет
- PHYSIOLOGY AND PATHOLOGY OF DEFECATIONДокумент57 страницPHYSIOLOGY AND PATHOLOGY OF DEFECATIONMonica BellyndaОценок пока нет
- Review of Related Literature of Jackfruit SeedДокумент4 страницыReview of Related Literature of Jackfruit SeedPrince Martin John Villamor80% (5)
- II. Anatomy and PhysiologyДокумент16 страницII. Anatomy and PhysiologyLee Cel100% (1)
- Intestinal ObstructionДокумент9 страницIntestinal ObstructionMuhammad Fuad Jaafar100% (1)
- PHYSICS Review Guide 2D Motion: M - L B NДокумент4 страницыPHYSICS Review Guide 2D Motion: M - L B Npotatoman51325Оценок пока нет
- Case Presentation (NCM 102)Документ26 страницCase Presentation (NCM 102)Ibs LimОценок пока нет
- RCOG Guidelines - Gestational Trophoblastic DiseaseДокумент12 страницRCOG Guidelines - Gestational Trophoblastic Diseasemob3100% (1)
- RCOG Guidelines - Gestational Trophoblastic DiseaseДокумент12 страницRCOG Guidelines - Gestational Trophoblastic Diseasemob3100% (1)
- ExtraДокумент3 страницыExtraaman100% (1)
- Formation Damage ExamplesДокумент89 страницFormation Damage ExamplesLaurensius Raymond SanjayaОценок пока нет
- Human digestive system overviewДокумент78 страницHuman digestive system overviewBerrak AydınОценок пока нет
- Chartering Terms ExplainedДокумент49 страницChartering Terms Explainedbrett1856Оценок пока нет
- Process Plant Layout - Seán Moran 1-2Документ2 страницыProcess Plant Layout - Seán Moran 1-2CunCunAlAndra100% (1)
- Constipation in ChildrenДокумент70 страницConstipation in ChildrendrhananfathyОценок пока нет
- HUMSS - Q3 - Trends - Mod5 - Global Networks Part 1Документ24 страницыHUMSS - Q3 - Trends - Mod5 - Global Networks Part 1Chernie Deroma Obsenares67% (6)
- To Perforasi GasterДокумент27 страницTo Perforasi GasterPuthu BelegugОценок пока нет
- Case Study of AmoebiasisДокумент7 страницCase Study of Amoebiasisbuzz Q75% (4)
- NCM 116 W1 Reading HandoutДокумент13 страницNCM 116 W1 Reading Handoutriza sarmientoОценок пока нет
- Gi NclexДокумент14 страницGi NclexYoke W Khoo100% (3)
- Plastics as a Building Material GuideДокумент24 страницыPlastics as a Building Material GuideVinod Nair100% (1)
- The Human Digestive System: Grade 10 Canadian Science Ossd Beijing Royal SchoolДокумент32 страницыThe Human Digestive System: Grade 10 Canadian Science Ossd Beijing Royal SchoolArnold Achilles Bautista Caccam100% (1)
- Abdominal Wall Defects: Omphalocele and Gastroschisis: DR - Enono Yhoshu Department of Pediatric SurgeryДокумент42 страницыAbdominal Wall Defects: Omphalocele and Gastroschisis: DR - Enono Yhoshu Department of Pediatric SurgeryYogi drОценок пока нет
- Sandvik H8800 Crusher Parts ManualДокумент3 страницыSandvik H8800 Crusher Parts ManualTomas Chien0% (1)
- Energy Engineering and Management For Building SystemДокумент288 страницEnergy Engineering and Management For Building SystemJivan BadaghaОценок пока нет
- Problem 5 GIT Group 12Документ126 страницProblem 5 GIT Group 12CindyОценок пока нет
- Problem 5 Git Aldi FДокумент158 страницProblem 5 Git Aldi Faldi firdausОценок пока нет
- Plenary 5B Group 13Документ163 страницыPlenary 5B Group 13Obet Agung 天Оценок пока нет
- Colonic LesionsДокумент89 страницColonic Lesionsjagadeesan_ushaОценок пока нет
- Gastrointestinal System Block Problem 3: Almira Nabila Valmai 405130193Документ79 страницGastrointestinal System Block Problem 3: Almira Nabila Valmai 405130193almira valmaiОценок пока нет
- Stoomach Anatomy PresentationДокумент112 страницStoomach Anatomy PresentationseniorhypeОценок пока нет
- Pemicu 5 GITДокумент52 страницыPemicu 5 GITMudita DewiОценок пока нет
- 2nd Problem PlenoДокумент92 страницы2nd Problem PlenoAlicia TjinОценок пока нет
- Fecal EliminationДокумент4 страницыFecal EliminationEzra MaeОценок пока нет
- Bahan Pemicu 3 Gastrointestinal Ivan BuntaraДокумент109 страницBahan Pemicu 3 Gastrointestinal Ivan BuntaraMarco GunawanОценок пока нет
- Askep Ca Colon: by Ns. Tiara, MNSДокумент37 страницAskep Ca Colon: by Ns. Tiara, MNSTiara Jauhara AzzahraОценок пока нет
- Plenary 3 Group 13Документ122 страницыPlenary 3 Group 13Obet Agung 天Оценок пока нет
- Stomach: Arterial SupplyДокумент13 страницStomach: Arterial SupplymariamОценок пока нет
- Digestive SystemДокумент54 страницыDigestive SystemChary Johanne MenesesОценок пока нет
- Lower GI Anatomy, Physiology and DisordersДокумент59 страницLower GI Anatomy, Physiology and DisordersAnonymous uvIS38c5vОценок пока нет
- Rectal Carcinoma.rДокумент4 страницыRectal Carcinoma.rRaf Kevin GelacioОценок пока нет
- Hirschsprung'S Disease OR Congenital Aganglionic MegacolonДокумент59 страницHirschsprung'S Disease OR Congenital Aganglionic MegacolonHarshika KDGОценок пока нет
- Assessment of AbdomenДокумент3 страницыAssessment of AbdomenAhmed EzzatОценок пока нет
- GS DivisionДокумент42 страницыGS DivisionDonald IDEDEОценок пока нет
- Amy Parrales Ruth’s lecture Gastrointestinal system Part I anatomyДокумент31 страницаAmy Parrales Ruth’s lecture Gastrointestinal system Part I anatomySean PitmanОценок пока нет
- Elimination PatternДокумент50 страницElimination Patternmamoonazafar2Оценок пока нет
- Diverticular DiseaseДокумент8 страницDiverticular Diseasenurse_enzo100% (1)
- G.I TractДокумент59 страницG.I Tractasifahamed51243Оценок пока нет
- Etiologi Dan Patofisiologi Bedah DigestifДокумент46 страницEtiologi Dan Patofisiologi Bedah DigestifNurul HidayatiОценок пока нет
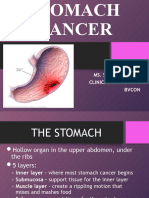
- Stomach CancerДокумент36 страницStomach CancerSonali DakhoreОценок пока нет
- Examination of Intestinal Obstruction, Acute Abdomen and Acute Appendicitis - Eugh & BwembyaДокумент29 страницExamination of Intestinal Obstruction, Acute Abdomen and Acute Appendicitis - Eugh & BwembyaForeighn97Оценок пока нет
- Gastrointestinal Fistula GuideДокумент60 страницGastrointestinal Fistula GuideSangija kamataОценок пока нет
- Git LecДокумент6 страницGit LecKim Sa-buОценок пока нет
- Physilogy Large IntestineДокумент23 страницыPhysilogy Large Intestinemohammed khalishОценок пока нет
- CancerДокумент30 страницCancerAbhirami BabuОценок пока нет
- Hirschsprung's Disease ExplainedДокумент11 страницHirschsprung's Disease ExplainedKarl JoseОценок пока нет
- Applied Aspect GITДокумент21 страницаApplied Aspect GITVivek RathiОценок пока нет
- Small & Large Intestines - LectureДокумент70 страницSmall & Large Intestines - Lecturehussain AltaherОценок пока нет
- Digestive and Gastrointestinal Function HandoutsДокумент15 страницDigestive and Gastrointestinal Function HandoutsChristine Joy FloresОценок пока нет
- Acute Gastroenteritis Causes, Symptoms, Diagnosis & TreatmentДокумент9 страницAcute Gastroenteritis Causes, Symptoms, Diagnosis & TreatmentJona Bruno100% (1)
- Hirsch SprungДокумент16 страницHirsch SprungjessyОценок пока нет
- Gastric CancerДокумент21 страницаGastric CancerTiffany AdriasОценок пока нет
- INTESTINEДокумент98 страницINTESTINEDeepika LingamОценок пока нет
- Class 7 (G1) - GI TractДокумент112 страницClass 7 (G1) - GI TractAdel mohammadОценок пока нет
- ColonosДокумент8 страницColonosHengki YongОценок пока нет
- Problem 3 GI Tract Group 13Документ159 страницProblem 3 GI Tract Group 13Alicia TjinОценок пока нет
- Digestive System PathophysiologyДокумент16 страницDigestive System PathophysiologyCamryn NewellОценок пока нет
- Lect 3 Disorder of Mouth and EsophagusДокумент42 страницыLect 3 Disorder of Mouth and EsophagusShayan ShayanОценок пока нет
- Problem 5 GIT Kelompok 16Документ116 страницProblem 5 GIT Kelompok 16Andreas AdiwinataОценок пока нет
- RLE B3 - Concept Map On Altered NutritionДокумент59 страницRLE B3 - Concept Map On Altered NutritionCARLOS JOSETON PAOLO SANTIAGO TORREОценок пока нет
- Week1 UgitДокумент119 страницWeek1 UgitriverabeanicoОценок пока нет
- Expansion Tank Design Guide, How To Size and Select An Expansion Tank For A Chilled Water System 1Документ1 страницаExpansion Tank Design Guide, How To Size and Select An Expansion Tank For A Chilled Water System 1CunCunAlAndraОценок пока нет
- Expansion Tank Design Guide, How To Size and Select An Expansion Tank For A Chilled Water System 2Документ1 страницаExpansion Tank Design Guide, How To Size and Select An Expansion Tank For A Chilled Water System 2CunCunAlAndraОценок пока нет
- Evaporative Condenser Engineering Manual: Technical ResourcesДокумент18 страницEvaporative Condenser Engineering Manual: Technical ResourcesMohamed IbrahimОценок пока нет
- Expansion Tank Design Guide, How To Size and Select An Expansion Tank For A Chilled Water System 3Документ1 страницаExpansion Tank Design Guide, How To Size and Select An Expansion Tank For A Chilled Water System 3CunCunAlAndraОценок пока нет
- Evaporative Condenser Engineering Manual: Technical ResourcesДокумент18 страницEvaporative Condenser Engineering Manual: Technical ResourcesMohamed IbrahimОценок пока нет
- GF Signet 515 2536 Manual02Документ1 страницаGF Signet 515 2536 Manual02CunCunAlAndraОценок пока нет
- Process Plant Layout - Seán Moran 3-4Документ2 страницыProcess Plant Layout - Seán Moran 3-4CunCunAlAndraОценок пока нет
- GF Signet 515 2536 Manual01Документ1 страницаGF Signet 515 2536 Manual01CunCunAlAndraОценок пока нет
- Evaporative Condenser Engineering Manual: Technical ResourcesДокумент18 страницEvaporative Condenser Engineering Manual: Technical ResourcesMohamed IbrahimОценок пока нет
- Safety Data Sheet for FAME (Fatty Acid Methyl EsterДокумент14 страницSafety Data Sheet for FAME (Fatty Acid Methyl EsterCunCunAlAndraОценок пока нет
- Consulting Business ModelДокумент1 страницаConsulting Business ModelCunCunAlAndraОценок пока нет
- Management Gathering 0718 - Distribution - v5 CoverДокумент1 страницаManagement Gathering 0718 - Distribution - v5 CoverCunCunAlAndraОценок пока нет
- 1348493956.2409obstetrics Handbook PDFДокумент48 страниц1348493956.2409obstetrics Handbook PDFdrng48Оценок пока нет
- NonalcoholicFattyLiverDisease2012 25762 FTPДокумент19 страницNonalcoholicFattyLiverDisease2012 25762 FTPbudi_26690Оценок пока нет
- MAPAX1Документ2 страницыMAPAX1CunCunAlAndraОценок пока нет
- Frontline Gastroenterol 2014 Dyson Flgastro 2013 100404Документ11 страницFrontline Gastroenterol 2014 Dyson Flgastro 2013 100404CunCunAlAndraОценок пока нет
- Gastro Enter Oh Epa ToДокумент29 страницGastro Enter Oh Epa TodeliaintanОценок пока нет
- Early Liver TransplantationДокумент11 страницEarly Liver TransplantationCunCunAlAndraОценок пока нет
- Pitri - GI.Pemicu 4. GE+ Tifus AbdominalisДокумент154 страницыPitri - GI.Pemicu 4. GE+ Tifus AbdominalisCunCunAlAndraОценок пока нет
- Kjae-68-101 Transfusion-Related Acute Lung InjuryДокумент5 страницKjae-68-101 Transfusion-Related Acute Lung InjuryCunCunAlAndraОценок пока нет
- Daftar Obat AnesДокумент44 страницыDaftar Obat AnesCunCunAlAndraОценок пока нет
- RicoДокумент62 страницыRicoCunCunAlAndraОценок пока нет
- RicoДокумент62 страницыRicoCunCunAlAndraОценок пока нет
- Presentation by Harshal Sethiya N Mitul UpadhyayДокумент26 страницPresentation by Harshal Sethiya N Mitul Upadhyaysanket jain100% (1)
- CT AC 72A<INV=<90A 70A<REC=<135A Part SpecДокумент7 страницCT AC 72A<INV=<90A 70A<REC=<135A Part SpecEdwin Mosos RamosОценок пока нет
- Balzac GaitДокумент7 страницBalzac Gaithieratic_headОценок пока нет
- UntreatedДокумент29 страницUntreatedhahahaОценок пока нет
- PDF If I Break 15 Portia Moore CompressДокумент61 страницаPDF If I Break 15 Portia Moore CompressAlbenis RodríguezОценок пока нет
- Air Preparation Products: Parker Pneumatic Section EДокумент11 страницAir Preparation Products: Parker Pneumatic Section EPartsGopher.comОценок пока нет
- Kisii University course explores environmental biotech, bioprocessingДокумент4 страницыKisii University course explores environmental biotech, bioprocessingRyan ReighnsОценок пока нет
- SSCM Roads and Bridges - Annex III Technical Specifications 105 C1 PDFДокумент254 страницыSSCM Roads and Bridges - Annex III Technical Specifications 105 C1 PDFSite Engineer.2p2100% (1)
- Meter Moving CoilДокумент4 страницыMeter Moving Coilabecdf100% (1)
- MM 361: Advanced Manufacturing: InstructionsДокумент3 страницыMM 361: Advanced Manufacturing: InstructionsSimLo Lulumani Ko'osiko Taloanimae'aОценок пока нет
- Safety Data Sheet: SECTION 1: Identification of The Substance/mixture and of The Company/ UndertakingДокумент10 страницSafety Data Sheet: SECTION 1: Identification of The Substance/mixture and of The Company/ UndertakingBradyОценок пока нет
- Small ScienceДокумент368 страницSmall Sciencereach27Оценок пока нет
- Seating Arrangement Rani MamДокумент44 страницыSeating Arrangement Rani Mamnagendra thelagariОценок пока нет
- Animal Talk Spring 09Документ32 страницыAnimal Talk Spring 09chuckc23Оценок пока нет
- Tuto Traktor Arduino enДокумент11 страницTuto Traktor Arduino enlexetaОценок пока нет
- BGMEA University of Fashion & Technology (BUFT)Документ9 страницBGMEA University of Fashion & Technology (BUFT)RIFAT HASANОценок пока нет
- Avl Tree Definition: Avl Trees Are Balanced Anavltreeisa Such That For Every Internal Node V of T, TheДокумент3 страницыAvl Tree Definition: Avl Trees Are Balanced Anavltreeisa Such That For Every Internal Node V of T, TheSumanta DattaОценок пока нет
- trs5 Key Cho Cac BanДокумент35 страницtrs5 Key Cho Cac BanNguyệt NgôОценок пока нет
- SPE 18184 OPUS: An Expert Advisor For Artificial LiftДокумент8 страницSPE 18184 OPUS: An Expert Advisor For Artificial Liftlepro brunelОценок пока нет