Вам также может понравиться
- Anatomy of The SpineДокумент61 страницаAnatomy of The SpineUlfiani Hidayah100% (1)
- Symmetry/ Asymmetry Deformity Torticolis Hematoma: InspeksiДокумент8 страницSymmetry/ Asymmetry Deformity Torticolis Hematoma: InspeksiUlfiani HidayahОценок пока нет
- Text Book Reading LumbalДокумент9 страницText Book Reading LumbalUlfiani HidayahОценок пока нет
- Fix Text Book ReadingДокумент58 страницFix Text Book ReadingUlfiani HidayahОценок пока нет
- Case Rereport Burs FractureДокумент39 страницCase Rereport Burs FractureUlfiani HidayahОценок пока нет
- Text Book Reading LumbalДокумент9 страницText Book Reading LumbalUlfiani HidayahОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Bomba - ITT - Família 3171Документ76 страницBomba - ITT - Família 3171UezilheiОценок пока нет
- Air & Space Law AssignmentДокумент5 страницAir & Space Law AssignmentPartha Mehrotra100% (1)
- TM 5-3805-291-23-1Документ1 520 страницTM 5-3805-291-23-1Advocate100% (1)
- First Aid Unit PlanДокумент27 страницFirst Aid Unit Planapi-497283129Оценок пока нет
- Llacer FdarДокумент2 страницыLlacer FdarRaidis PangilinanОценок пока нет
- Thoracic Hinge - Edited8.1.15 PDFДокумент5 страницThoracic Hinge - Edited8.1.15 PDFnambaccucОценок пока нет
- Biers BlockДокумент4 страницыBiers Blockemkay1234Оценок пока нет
- Radiall Et. Al. v. GlenairДокумент12 страницRadiall Et. Al. v. GlenairPriorSmartОценок пока нет
- EC270Документ13 страницEC270AmilmcОценок пока нет
- Paediatric Guidelines TorticollisДокумент4 страницыPaediatric Guidelines TorticollisCatalin ChiriloiОценок пока нет
- Mr. SkeletonДокумент6 страницMr. SkeletonKarthika Paul100% (1)
- Care of Patients With TractionДокумент25 страницCare of Patients With Tractionmftaganas100% (1)
- Neuro Sensory AssessmentДокумент46 страницNeuro Sensory AssessmentPrecious SantayanaОценок пока нет
- SG125HV V1 UEN Ver14 202002Документ106 страницSG125HV V1 UEN Ver14 202002MaruОценок пока нет
- Bitts Park Risk AssessmentДокумент4 страницыBitts Park Risk Assessmentapi-339095212Оценок пока нет
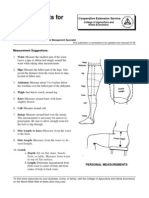
- Measurements For Fitting Pants: Guide C-209Документ2 страницыMeasurements For Fitting Pants: Guide C-209Ranil Hashan FОценок пока нет
- Ch-8 Body Movements - Day1Документ12 страницCh-8 Body Movements - Day1dr satnam kaurОценок пока нет
- Structure in The Kite RunnerДокумент4 страницыStructure in The Kite Runnerushi12Оценок пока нет
- Risk Assessment For Ceramic & Porcelain Tile WorksДокумент6 страницRisk Assessment For Ceramic & Porcelain Tile WorksFaizan Tanveer100% (1)
- Bioptron Biology 1Документ6 страницBioptron Biology 1Nick100% (1)
- Sketetal SystemДокумент11 страницSketetal SystemBryan JagroopОценок пока нет
- Affidavit Complaint Slight Physical InjuryДокумент2 страницыAffidavit Complaint Slight Physical Injuryduanepo100% (1)
- Chest TraumaДокумент115 страницChest TraumaЕвгений ХанькоОценок пока нет
- Cerebral Blood Flow & StrokeДокумент35 страницCerebral Blood Flow & Stroke-'Henri Djhevon Kaary'-Оценок пока нет
- Respiration PHYSIOДокумент23 страницыRespiration PHYSIOTauseef AfridiОценок пока нет
- PE03 Midterm Week 3 ModuleДокумент6 страницPE03 Midterm Week 3 ModuleCorn FlakesОценок пока нет
- Difference Between 300 and 299Документ3 страницыDifference Between 300 and 299vedanth saiОценок пока нет
- OZ 02 The Marvelous Land of OzДокумент62 страницыOZ 02 The Marvelous Land of Ozbunnycat666Оценок пока нет
- Midea MSV1 07 09 12HRN1 CRN1Документ37 страницMidea MSV1 07 09 12HRN1 CRN1Giselma ZéoОценок пока нет
- Jigy WirgleДокумент486 страницJigy Wirglesierleinad1Оценок пока нет