Вам также может понравиться
- Now 1&refreqid Excelsior:&seq 4#pa Ge - Scan - Tab - ContentsДокумент5 страницNow 1&refreqid Excelsior:&seq 4#pa Ge - Scan - Tab - ContentsJANNIE BELLE RODRIGUEZОценок пока нет
- Errors of RefractionДокумент38 страницErrors of RefractionMohd RafiОценок пока нет
- Segmen Anterior Drawing: Edited by Dr. Franky F Sihombing, FKUSU2001Документ11 страницSegmen Anterior Drawing: Edited by Dr. Franky F Sihombing, FKUSU2001Franky Frans SihombingОценок пока нет
- Incomitant SquintДокумент41 страницаIncomitant Squintshreeja maheshwari100% (3)
- 15 Slit Lamp Biomicroscopy 2Документ36 страниц15 Slit Lamp Biomicroscopy 2Sri Rama Chandra ManchikantyОценок пока нет
- First Aid Q&A PDFДокумент764 страницыFirst Aid Q&A PDFStephanie Williams100% (9)
- Pa 1 Persuasive EssayДокумент4 страницыPa 1 Persuasive Essayapi-458023500Оценок пока нет
- Parasites, How To Eliminate Them NaturallyДокумент44 страницыParasites, How To Eliminate Them NaturallyXuxuxel100% (3)
- Epidemiology: Subject-Community Health NursingДокумент30 страницEpidemiology: Subject-Community Health NursingBabita Dhruw100% (3)
- Ocular TraumaДокумент50 страницOcular TraumafatimaОценок пока нет
- Ocular EmergenciesДокумент26 страницOcular EmergenciesYukianesa100% (1)
- Ocular Injuries and EmergenciesДокумент60 страницOcular Injuries and Emergenciesarnol3090100% (1)
- Refraction 2Документ47 страницRefraction 2RuDy RaviОценок пока нет
- Roving Ring ScotomaДокумент3 страницыRoving Ring ScotomaDeboprasad DasОценок пока нет
- Corneal Ulcer: Prepared By: Renuka Shrestha Roll No: 29 PBBN 3rd Year SMTCДокумент41 страницаCorneal Ulcer: Prepared By: Renuka Shrestha Roll No: 29 PBBN 3rd Year SMTCsushma shresthaОценок пока нет
- StrabismusДокумент31 страницаStrabismusalma palupi100% (1)
- Retinal Drawing A Lost Art of MedicineДокумент3 страницыRetinal Drawing A Lost Art of MedicinekavyaОценок пока нет
- Ocular Emergencies CMEДокумент35 страницOcular Emergencies CMEAmir Izzuddin SuibОценок пока нет
- Corneal UlcerДокумент21 страницаCorneal UlcerarturocerpaОценок пока нет
- Ocular EmergenciesДокумент38 страницOcular EmergenciesHaania KhanОценок пока нет
- StrabismusДокумент27 страницStrabismuspason1988Оценок пока нет
- Hyphema 2Документ7 страницHyphema 2heidyОценок пока нет
- Congenital CataractДокумент40 страницCongenital CataractRaymonde UyОценок пока нет
- Introduction To Low VisionДокумент15 страницIntroduction To Low VisionHira AtifОценок пока нет
- Corneal Ulcers in General Practice: Clinical IntelligenceДокумент2 страницыCorneal Ulcers in General Practice: Clinical IntelligenceBenitaОценок пока нет
- 2735 Pediatric Cataract Manual - CompressedДокумент66 страниц2735 Pediatric Cataract Manual - CompressedKevin RamsahaiОценок пока нет
- Diseases of Lens DR D.JLДокумент113 страницDiseases of Lens DR D.JLNithya GunasekaranОценок пока нет
- Fundus ExaminationДокумент43 страницыFundus Examinationsamuelpnrj25100% (2)
- RvoДокумент43 страницыRvoOrchlon LkОценок пока нет
- Ophtha SGD 1Документ4 страницыOphtha SGD 1Richelle IgnacioОценок пока нет
- AAO - External Disease and CorneaДокумент19 страницAAO - External Disease and CorneaJohn Paul VillaflorОценок пока нет
- Macular HoleДокумент80 страницMacular HoleRaissaОценок пока нет
- Applied Anatomy and Physiology of CorneaДокумент116 страницApplied Anatomy and Physiology of CorneaJoubertnassif100% (1)
- I Notes StrabismusДокумент92 страницыI Notes StrabismusPrincess EzzlynnОценок пока нет
- Common Eye Problems and DiagnosisДокумент84 страницыCommon Eye Problems and Diagnosisvivekrajbhilai5850Оценок пока нет
- CPG 5Документ29 страницCPG 5Budio SatyaОценок пока нет
- Orbital CellulitisДокумент21 страницаOrbital CellulitisElsa Octavia100% (1)
- Fluoresce in in OphthalmologyДокумент19 страницFluoresce in in OphthalmologyThingujam JamesОценок пока нет
- Periorbital and Orbital CellulitisДокумент51 страницаPeriorbital and Orbital CellulitisJoanne BlancoОценок пока нет
- Crao PosterДокумент1 страницаCrao PosterNataShini RajaRatnamОценок пока нет
- Hordeolum & ChalazionДокумент22 страницыHordeolum & ChalazionDion Satriawan Dhaniardi100% (1)
- Classification of Ptosis: 1. NeurogenicДокумент25 страницClassification of Ptosis: 1. NeurogenicMuliany PratiwiОценок пока нет
- Clinical OpticsДокумент88 страницClinical OpticsKris ArchibaldОценок пока нет
- Surgical Management of Senile CataractДокумент39 страницSurgical Management of Senile CataractKarthik ChellaОценок пока нет
- Thesis Protocol For M.S. Degree (Ophthalmology)Документ31 страницаThesis Protocol For M.S. Degree (Ophthalmology)zebaОценок пока нет
- Short Case PterygiumДокумент21 страницаShort Case PterygiumRSОценок пока нет
- Refractive ErrorsДокумент73 страницыRefractive ErrorsAnggunBW100% (1)
- Tele-Ophthalmology: By-Abhishek Yadav Optometrist Dr. R.P. Centre For Ophthalmic Sciences AiimsДокумент11 страницTele-Ophthalmology: By-Abhishek Yadav Optometrist Dr. R.P. Centre For Ophthalmic Sciences AiimsAbhishek Yadav0% (1)
- Ophtha Case ReportДокумент17 страницOphtha Case ReportJoy Mae Ann PeraltaОценок пока нет
- Ophthalmology Revision LectureДокумент80 страницOphthalmology Revision LectureCarla LaniganОценок пока нет
- Short Case 1 PterygiumДокумент15 страницShort Case 1 PterygiumAnmol KhadkaОценок пока нет
- TrichiasisДокумент9 страницTrichiasisMiftahThariq100% (1)
- BlepharitisДокумент11 страницBlepharitismohamadОценок пока нет
- Ocular Surface DiseaseДокумент82 страницыOcular Surface DiseaseRuth AntolinОценок пока нет
- Okap Samson Uveitis PDFДокумент12 страницOkap Samson Uveitis PDFsharu4291Оценок пока нет
- Diseases of Retina: The 4th Affilitated Hospital of China Medical University Eye Hospital of China Medical UniversityДокумент76 страницDiseases of Retina: The 4th Affilitated Hospital of China Medical University Eye Hospital of China Medical UniversityIcha NathaniaОценок пока нет
- The Pathophysiology and Treatment of Glaucoma PDFДокумент22 страницыThe Pathophysiology and Treatment of Glaucoma PDFNurul Dwi LestariОценок пока нет
- Anisometropia in Children and Its ProblemДокумент37 страницAnisometropia in Children and Its ProblemekaОценок пока нет
- Ophthalmic EmergencyДокумент17 страницOphthalmic EmergencyMohammad HelalОценок пока нет
- Lens and CataractДокумент55 страницLens and CataractRold Brio Sos100% (1)
- Case Based Ophthalmology GuideДокумент12 страницCase Based Ophthalmology GuideGradestack100% (2)
- Uveitis PDFДокумент17 страницUveitis PDFkmiz85Оценок пока нет
- 19 Rationale of Retinal Detachment ManagementДокумент87 страниц19 Rationale of Retinal Detachment ManagementvajasaОценок пока нет
- Topic Wise DNB Question BankДокумент30 страницTopic Wise DNB Question Bankritesh100% (1)
- Complication of Blood TransfusionДокумент5 страницComplication of Blood TransfusionChey Ochy ApriliaОценок пока нет
- Maintaining Balance: The Vestibular SystemДокумент28 страницMaintaining Balance: The Vestibular SystemMohammad Farouq OmarОценок пока нет
- Nejmoa1911998 PDFДокумент11 страницNejmoa1911998 PDFStella NoviaОценок пока нет
- HSSP Iii 2010Документ121 страницаHSSP Iii 2010eriasleОценок пока нет
- 1a-History Taking in SurgeryДокумент19 страниц1a-History Taking in SurgeryMohammad Farouq Omar100% (1)
- Disorders of ThoughtДокумент22 страницыDisorders of ThoughtMohammad Farouq OmarОценок пока нет
- Tanzania One Plan IIДокумент142 страницыTanzania One Plan IIMohammad Farouq OmarОценок пока нет
- Principles of Managing Severe Acute MalnutritionДокумент31 страницаPrinciples of Managing Severe Acute MalnutritionMohammad Farouq OmarОценок пока нет
- Eset PassДокумент1 страницаEset PassMohammad Farouq OmarОценок пока нет
- Sharpened One Plan - 2014Документ61 страницаSharpened One Plan - 2014Mohammad Farouq OmarОценок пока нет
- GynecologyДокумент56 страницGynecologyMohammad Farouq OmarОценок пока нет
- Muscle ExplainationДокумент66 страницMuscle ExplainationMohammad Farouq OmarОценок пока нет
- GynecologyДокумент56 страницGynecologyMohammad Farouq OmarОценок пока нет
- Aging (Senescence) 1Документ11 страницAging (Senescence) 1Mohammad Farouq OmarОценок пока нет
- ATrial FibrillationДокумент21 страницаATrial FibrillationMohammad Farouq OmarОценок пока нет
- Lahore MedicalДокумент12 страницLahore MedicalMohammad Farouq OmarОценок пока нет
- Lahore MedicalДокумент12 страницLahore MedicalMohammad Farouq OmarОценок пока нет
- 10 ArthropodДокумент40 страниц10 ArthropodMohammad Farouq OmarОценок пока нет
- Planning NotesДокумент55 страницPlanning NotesMohammad Farouq OmarОценок пока нет
- Cohort Studies: Mmbaga Ej. (MD, PHD) Department of Epidemiology and Biostatistics, MuhasДокумент23 страницыCohort Studies: Mmbaga Ej. (MD, PHD) Department of Epidemiology and Biostatistics, MuhasMohammad Farouq OmarОценок пока нет
- Entry Form: Hospital Best Practices in Infection Prevention and Control Awards Year ViДокумент1 страницаEntry Form: Hospital Best Practices in Infection Prevention and Control Awards Year ViPeepsОценок пока нет
- Soal Dan Pembahasan UN Bahasa Inggris SMA IPS 2009-2010Документ15 страницSoal Dan Pembahasan UN Bahasa Inggris SMA IPS 2009-2010Genius Edukasi50% (2)
- The Life Cycle of A Pandemic Crisis - Sars Impact On Air TravelДокумент17 страницThe Life Cycle of A Pandemic Crisis - Sars Impact On Air TravelGabriel Charles Lim PkОценок пока нет
- Outbreak Student Worksheet AnswersДокумент9 страницOutbreak Student Worksheet AnswersArlie Espeña DucducanОценок пока нет
- Appendicitis - Wikipedia, The Free EncyclopediaДокумент14 страницAppendicitis - Wikipedia, The Free EncyclopediaIchalAz100% (1)
- Comparison of Goldmann Applanation Tonometer, Tono-PenДокумент19 страницComparison of Goldmann Applanation Tonometer, Tono-PenLidiasilambaОценок пока нет
- Navel DisplacementДокумент4 страницыNavel Displacementdinesh100% (1)
- Common Diseases and Epidemics: PolioДокумент7 страницCommon Diseases and Epidemics: PolioTheAwein ChannelОценок пока нет
- Iec DengueДокумент3 страницыIec DengueKeith Wesley YbutОценок пока нет
- Skoda Corretto Barley Glucans Obesity08Документ2 страницыSkoda Corretto Barley Glucans Obesity08bcs002Оценок пока нет
- Cor PulmonaleДокумент15 страницCor PulmonaleRizky Zulfa Afrida100% (1)
- Daftar PustakaДокумент2 страницыDaftar PustakaYuli ErmaОценок пока нет
- NeurosyphilisДокумент2 страницыNeurosyphiliserfОценок пока нет
- Clinical and Microbiological Effect of Linezolid On Methicillin-ResistantДокумент10 страницClinical and Microbiological Effect of Linezolid On Methicillin-ResistantNoha GamalОценок пока нет
- GlomerulopatiДокумент16 страницGlomerulopatiFitri Murpiana MuntheОценок пока нет
- Part A-12-Wood Dust Allergies - Q&AДокумент8 страницPart A-12-Wood Dust Allergies - Q&Afernanda1rondelliОценок пока нет
- Clinical Features, Evaluation, and Diagnosis of Sepsis in Term and Late Preterm Infants PDFДокумент27 страницClinical Features, Evaluation, and Diagnosis of Sepsis in Term and Late Preterm Infants PDFJonathan WelchОценок пока нет
- A Development Disaster: HIV/AIDS As A Cause and Consequence of PovertyДокумент28 страницA Development Disaster: HIV/AIDS As A Cause and Consequence of Povertyago87100% (1)
- News ItemДокумент7 страницNews ItemnadiazakyfadillahОценок пока нет
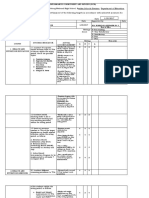
- Jen Ipcr 1st QuarterДокумент4 страницыJen Ipcr 1st QuarterJairolla ObayОценок пока нет
- Is The Cardiac Rehabilitation Programme Successful in Serdang Hospital: Patients' PerspectiveДокумент3 страницыIs The Cardiac Rehabilitation Programme Successful in Serdang Hospital: Patients' PerspectiveAnanthankumar MunusamyОценок пока нет
- UntitledДокумент4 страницыUntitledRafsan HossainОценок пока нет
- Zika (1) InfografiaДокумент2 страницыZika (1) Infografiaandrea lula da silvaОценок пока нет
- Water MicrobiologyДокумент15 страницWater MicrobiologyDayledaniel SorvetoОценок пока нет
- Chicken Pox and Herpes ZosterfinalДокумент31 страницаChicken Pox and Herpes ZosterfinalBinayaОценок пока нет
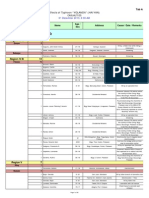
- List of Casualties Due To Typhoon YolandaДокумент31 страницаList of Casualties Due To Typhoon YolandaSunStar Philippine NewsОценок пока нет