Вам также может понравиться
- Medical History (General) : Subject Initials Subject ID DateДокумент1 страницаMedical History (General) : Subject Initials Subject ID Datewahyu_sitaОценок пока нет
- ReadmeДокумент3 страницыReadmeYuares B EyjafjallajoekullОценок пока нет
- New Doc 2018-05-21Документ16 страницNew Doc 2018-05-21wahyu_sitaОценок пока нет
- 1 DemografiДокумент2 страницы1 Demografiwahyu_sitaОценок пока нет
- Daftar Pustaka S2 WhyДокумент7 страницDaftar Pustaka S2 Whywahyu_sitaОценок пока нет
- 1445 Gruenwald CДокумент21 страница1445 Gruenwald Cwahyu_sitaОценок пока нет
- BPI Okt - JunaidiДокумент28 страницBPI Okt - Junaidiwahyu_sitaОценок пока нет
- Usg Muskuloskel in Oa Hand 2016Документ3 страницыUsg Muskuloskel in Oa Hand 2016wahyu_sitaОценок пока нет
- Bell's PalsyДокумент37 страницBell's Palsywahyu_sitaОценок пока нет
- The Mayo Elbow Performance Score PDFДокумент1 страницаThe Mayo Elbow Performance Score PDFwahyu_sitaОценок пока нет
- Usg Muskuloskel in Oa Hand 2016Документ3 страницыUsg Muskuloskel in Oa Hand 2016wahyu_sitaОценок пока нет
- Suplemen AmputeeДокумент59 страницSuplemen Amputeewahyu_sitaОценок пока нет
- TheoryДокумент8 страницTheorywahyu_sitaОценок пока нет
- Energy Expenditure During Walking JoggingДокумент19 страницEnergy Expenditure During Walking Joggingwahyu_sitaОценок пока нет
- OA SourceДокумент81 страницаOA Sourcewahyu_sitaОценок пока нет
- Koos EnglishДокумент4 страницыKoos EnglishJulie MayoОценок пока нет
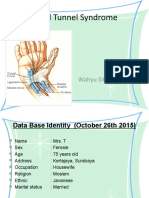
- CTSДокумент24 страницыCTSwahyu_sitaОценок пока нет
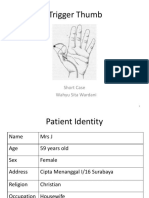
- Trigger ThumbДокумент21 страницаTrigger Thumbwahyu_sitaОценок пока нет
- Osteoarthritis Genu: Short Case Wahyu Sita WardaniДокумент52 страницыOsteoarthritis Genu: Short Case Wahyu Sita Wardaniwahyu_sitaОценок пока нет
- Tennis ElbowДокумент23 страницыTennis Elbowwahyu_sitaОценок пока нет
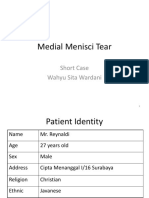
- Medial Menisci Tear: Short Case Wahyu Sita WardaniДокумент25 страницMedial Menisci Tear: Short Case Wahyu Sita Wardaniwahyu_sitaОценок пока нет
- Impengement SyndromeДокумент39 страницImpengement Syndromewahyu_sitaОценок пока нет
- Bell''s PalsyДокумент54 страницыBell''s Palsywahyu_sitaОценок пока нет
- Impengement SyndromeДокумент39 страницImpengement Syndromewahyu_sitaОценок пока нет
- Berg Balance Scale PDFДокумент4 страницыBerg Balance Scale PDFThereseОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- Animal Testing: Pros and ConsДокумент5 страницAnimal Testing: Pros and ConsSheryl UrieОценок пока нет
- Delivery of CH ServicesДокумент39 страницDelivery of CH ServicesAnand gowdaОценок пока нет
- Principales Fluidos y Secreciones de Análisis en LaboratorioДокумент34 страницыPrincipales Fluidos y Secreciones de Análisis en LaboratorioDennis Lorena Cárdenas LealОценок пока нет
- What Are The Classification of HospitalsДокумент11 страницWhat Are The Classification of HospitalsLily Jane PakiwonОценок пока нет
- Children Hypertension ChartДокумент4 страницыChildren Hypertension ChartHo Yoke MeiОценок пока нет
- Professor: Submitted To: Ms. Mary Grace L. SagunДокумент7 страницProfessor: Submitted To: Ms. Mary Grace L. SagunlalaОценок пока нет
- Attitude Towards Second Hand Smoke, Smoking and QuitingДокумент5 страницAttitude Towards Second Hand Smoke, Smoking and QuitingBaonganОценок пока нет
- 1118005I Rev. 02Документ2 страницы1118005I Rev. 02BalesheОценок пока нет
- HZ Dental CatalogueДокумент217 страницHZ Dental Cataloguemaggeorge1Оценок пока нет
- Ref - ECC RHS-Phase-2-articleДокумент10 страницRef - ECC RHS-Phase-2-articlePROF. ERWIN M. GLOBIO, MSITОценок пока нет
- Williams2014Документ10 страницWilliams2014Eugeni Llorca BordesОценок пока нет
- Bioregulatory Medicine History - Reinhold VollДокумент11 страницBioregulatory Medicine History - Reinhold VollD.W. Smith100% (2)
- Report Chapter 3Документ16 страницReport Chapter 3JUNE MARK CRUZОценок пока нет
- Quiz No.1Документ5 страницQuiz No.1Charina AubreyОценок пока нет
- Statement of Purpose (Clinical Dermatology-MSc) Cardiff UniversityДокумент3 страницыStatement of Purpose (Clinical Dermatology-MSc) Cardiff UniversitySheikh Shafiq Siam100% (1)
- English For Academic and Professional Purposes: Quarter 1 - Module 2 Text StructureДокумент25 страницEnglish For Academic and Professional Purposes: Quarter 1 - Module 2 Text StructureBeverly Joy BragaisОценок пока нет
- Project Based Learning Part IIДокумент21 страницаProject Based Learning Part IIcrismedionaОценок пока нет
- Grade 9 Science Biology 1 DLPДокумент13 страницGrade 9 Science Biology 1 DLPManongdo AllanОценок пока нет
- English For Nurse 5: 5. Reading Unit A. MR Jansen Has Had A Myocardial InfarctionДокумент4 страницыEnglish For Nurse 5: 5. Reading Unit A. MR Jansen Has Had A Myocardial InfarctiondnnssnОценок пока нет
- Essentials of Orthodontics PDFДокумент591 страницаEssentials of Orthodontics PDFKENAN ABBARA100% (1)
- Surveillance and Outbreak Investigation StudentДокумент11 страницSurveillance and Outbreak Investigation Studentnura meccaОценок пока нет
- Silencing Tumor Suppressor Genes OncogenesДокумент1 страницаSilencing Tumor Suppressor Genes OncogenesEnkhbaatar BatmagnaiОценок пока нет
- Artikel Ilmiah (PKL) MiaДокумент10 страницArtikel Ilmiah (PKL) MiaKrismarita HandayaniОценок пока нет
- Unit 1 Good Morning, NurseДокумент12 страницUnit 1 Good Morning, NurseAkun NyampahОценок пока нет
- Ace Score Resilience Q 2Документ5 страницAce Score Resilience Q 2KhadijaAnamОценок пока нет
- Pathophysiology - CholedocholithiasisДокумент1 страницаPathophysiology - CholedocholithiasisMark OrculloОценок пока нет
- Thrombolytic TherapyДокумент24 страницыThrombolytic TherapyJayarani Ashok100% (1)
- Epidemiology - AMBOSSДокумент13 страницEpidemiology - AMBOSSFlowerОценок пока нет
- Avika ReportДокумент2 страницыAvika ReportChinish KalraОценок пока нет
- Care Plan - Fluid OverloadДокумент1 страницаCare Plan - Fluid Overloadelysen01Оценок пока нет