Вам также может понравиться
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- Body Systems (Grade 6) - Free Printable Tests and Worksheets - HelpTeachingДокумент1 страницаBody Systems (Grade 6) - Free Printable Tests and Worksheets - HelpTeachingshuganesh82% (11)
- Medical Coding 1 - 2 Study GuideДокумент41 страницаMedical Coding 1 - 2 Study GuideAnthony Martinez75% (4)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Cupping Therapy ExplainedДокумент16 страницCupping Therapy ExplainedAbdul Rahman Khan100% (3)
- Ivan P. Casserly MB BCH, Ravish Sachar MD, Jay S. Yadav MD - Practical Peripheral Vascular Intervention-LWW (2011)Документ478 страницIvan P. Casserly MB BCH, Ravish Sachar MD, Jay S. Yadav MD - Practical Peripheral Vascular Intervention-LWW (2011)Xunyao LuОценок пока нет
- Circulatory System Multiple Choice QuestionsДокумент4 страницыCirculatory System Multiple Choice QuestionsAlee MubeenОценок пока нет
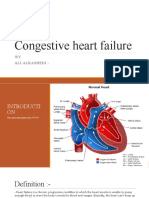
- CHF: Congestive Heart Failure Causes, Symptoms & TreatmentДокумент13 страницCHF: Congestive Heart Failure Causes, Symptoms & Treatmentali alrashediОценок пока нет
- Case Based Pediatrics For Medical Students and ResidentsДокумент6 страницCase Based Pediatrics For Medical Students and Residentssantosaerwin6591100% (1)
- Physio Ex Exercise 6 Activity 1Документ3 страницыPhysio Ex Exercise 6 Activity 1Roland Calipayan Jr.Оценок пока нет
- Multiple Choice Questions and AnsДокумент10 страницMultiple Choice Questions and Ansqudsia_niazi100% (1)
- HemofiliaДокумент1 страницаHemofilianafisyarifahОценок пока нет
- Disaster Victims IdentificationДокумент1 страницаDisaster Victims IdentificationnafisyarifahОценок пока нет
- Topic of Lectures (Critical Appraisal Module) : NO Topik Pengampu JAMДокумент4 страницыTopic of Lectures (Critical Appraisal Module) : NO Topik Pengampu JAMnafisyarifahОценок пока нет
- Presentation 1Документ7 страницPresentation 1nafisyarifahОценок пока нет
- Diagnosis WorksheetДокумент2 страницыDiagnosis Worksheetnurul ramadhanyОценок пока нет
- PJ KritikalДокумент38 страницPJ KritikalnafisyarifahОценок пока нет
- 1 Outbreak InvestigationДокумент48 страниц1 Outbreak InvestigationAbdul Charis Konoras100% (1)
- Presus GravesДокумент1 страницаPresus GravesnafisyarifahОценок пока нет
- Materi MCQ Blok 17Документ2 страницыMateri MCQ Blok 17DwiFajarwatiPrayitnoОценок пока нет
- MCQ 1 Dan MCQ 2Документ3 страницыMCQ 1 Dan MCQ 2nafisyarifahОценок пока нет
- Journal ReadingДокумент18 страницJournal ReadingnafisyarifahОценок пока нет
- Dr. Yuliaji Narendra Putra, SpB Fluid Therapy GuideДокумент36 страницDr. Yuliaji Narendra Putra, SpB Fluid Therapy GuidenafisyarifahОценок пока нет
- Trypanosoma. Blok 15Документ60 страницTrypanosoma. Blok 15nafisyarifahОценок пока нет
- Gangguan Pada Pembuluh Darah: DR - Dr.zaenal M. Sofro, AIFM, Sport & Circ. Med. Bagian Ilmu Faal Fak - Kedokteran UGMДокумент68 страницGangguan Pada Pembuluh Darah: DR - Dr.zaenal M. Sofro, AIFM, Sport & Circ. Med. Bagian Ilmu Faal Fak - Kedokteran UGMnafisyarifahОценок пока нет
- Meningoensefalitis-Fk Umy 2015Документ39 страницMeningoensefalitis-Fk Umy 2015nafisyarifahОценок пока нет
- Update On Perioperative Fluid Therapy DR Y Narendra, SPBДокумент36 страницUpdate On Perioperative Fluid Therapy DR Y Narendra, SPBnafisyarifahОценок пока нет
- Meningitis 2005Документ87 страницMeningitis 2005nafisyarifahОценок пока нет
- TBI ZamДокумент67 страницTBI ZamnafisyarifahОценок пока нет
- MeningismДокумент4 страницыMeningismnafisyarifahОценок пока нет
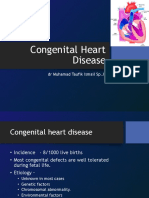
- CHD, VHD, CP, Ie - TaufikДокумент76 страницCHD, VHD, CP, Ie - Taufikirawati hidayahОценок пока нет
- Dr. Yuliaji Narendra Putra, SpB Fluid Therapy GuideДокумент36 страницDr. Yuliaji Narendra Putra, SpB Fluid Therapy GuidenafisyarifahОценок пока нет
- DM NafiДокумент11 страницDM NafinafisyarifahОценок пока нет
- Perioperative Nutrition Post Laparotomy PatientДокумент19 страницPerioperative Nutrition Post Laparotomy PatientnafisyarifahОценок пока нет
- ACE I ARBsДокумент23 страницыACE I ARBsnafisyarifahОценок пока нет
- Endocrine System DiseasesДокумент87 страницEndocrine System DiseasesFahmiArifMuhammadОценок пока нет
- Likelihood Ratio Dan NormogramДокумент3 страницыLikelihood Ratio Dan NormogramKenZie DenendraОценок пока нет
- Asthma Cop DДокумент123 страницыAsthma Cop DnafisyarifahОценок пока нет
- Radiology Examination of Thorax-2011 PDFДокумент16 страницRadiology Examination of Thorax-2011 PDFGanang Azhar GuntaraОценок пока нет
- Preoperative Physiology, Imaging, andДокумент13 страницPreoperative Physiology, Imaging, andSiLfia SahrinОценок пока нет
- Mfine CardiologistsДокумент7 страницMfine Cardiologistsmfine healthОценок пока нет
- NCM 118 L 3rd ExamДокумент3 страницыNCM 118 L 3rd Examj UОценок пока нет
- 4 - Toronto Notes 2011 - Cardiology - and - Cardiovascular - SurgeryДокумент60 страниц4 - Toronto Notes 2011 - Cardiology - and - Cardiovascular - Surgeryqobsar100% (1)
- 1102 OBJECTIVE 2 PBL 2 Cardiac Cycle .Документ3 страницы1102 OBJECTIVE 2 PBL 2 Cardiac Cycle .brennan12345Оценок пока нет
- Science Form 3 Chapter 3 TestДокумент7 страницScience Form 3 Chapter 3 TestShatviga VisvalingamОценок пока нет
- OK - Modul Ortho - Bone Cement Implantation SyndromeДокумент18 страницOK - Modul Ortho - Bone Cement Implantation SyndromeWanditoGayuhUtomoОценок пока нет
- EECP IabpДокумент16 страницEECP IabpMythily VedhagiriОценок пока нет
- Computational Models For The Human Body PDFДокумент679 страницComputational Models For The Human Body PDFGuilherme AyresОценок пока нет
- Dwnload Full Ekg Plain and Simple 3rd Edition Ellis Test Bank PDFДокумент7 страницDwnload Full Ekg Plain and Simple 3rd Edition Ellis Test Bank PDFpeterrodriguezcwbqomdksi100% (10)
- Programbook IsicamДокумент36 страницProgrambook Isicamadi bestaraОценок пока нет
- RPT: Science Form 3Документ15 страницRPT: Science Form 3Ani AhwaiОценок пока нет
- Icu NCP 2Документ2 страницыIcu NCP 2James Casauran LandagoraОценок пока нет
- Chapter 11 The Cardiovascular SystemДокумент25 страницChapter 11 The Cardiovascular SystemYeshia InocencioОценок пока нет
- IV TagДокумент1 страницаIV TagJonathan delos ReyesОценок пока нет
- Diuretic Usage in Chronic Heart Failure PatientДокумент1 страницаDiuretic Usage in Chronic Heart Failure Patientmuh_alatas40Оценок пока нет
- Cardiology Lectures 1 4 DR - Deduyo PDFДокумент31 страницаCardiology Lectures 1 4 DR - Deduyo PDFMiguel Cuevas DolotОценок пока нет
- Acute Decompensated HeartДокумент7 страницAcute Decompensated HeartRay MartínezОценок пока нет
- Tata Laksana Perawatan Gigi Pada Pasien Kelainan Jantung Yang Ditanamkan Icd Dan Mengonsumsi WarfarinДокумент17 страницTata Laksana Perawatan Gigi Pada Pasien Kelainan Jantung Yang Ditanamkan Icd Dan Mengonsumsi WarfarinEka ApriantiОценок пока нет
- Congenital heart disease overviewДокумент8 страницCongenital heart disease overviewgolagani praveenkumarОценок пока нет
- What is BiologyДокумент33 страницыWhat is BiologySA - 10WB 933839 The Woodlands SSОценок пока нет
- Aortic RegurgitationДокумент16 страницAortic Regurgitationrobby zayendraОценок пока нет