Вам также может понравиться
- Management of Acute Coronary SyndromeДокумент73 страницыManagement of Acute Coronary SyndromeSantosh NaliathОценок пока нет
- ECG Changes in ACSДокумент39 страницECG Changes in ACSnavenОценок пока нет
- Stemi PDFДокумент60 страницStemi PDFPraveen100% (1)
- DR Supartono-ECG DiagnosisДокумент85 страницDR Supartono-ECG DiagnosisvinahandoyoОценок пока нет
- Normal Ecg, Infarction & Arrhythmia SДокумент98 страницNormal Ecg, Infarction & Arrhythmia SAdinda GupitaОценок пока нет
- Acs PPT Final 6-14-10Документ66 страницAcs PPT Final 6-14-10Joel_Ang_Ibasc_4318Оценок пока нет
- CAD Investigation, Management and ComplicationsДокумент13 страницCAD Investigation, Management and Complicationsrazan.girl.2010Оценок пока нет
- Acute Coronary SindromeДокумент59 страницAcute Coronary SindromeRhenty NarusОценок пока нет
- Normal Ecg, Infarction & Arrhythmias: Iqbal Lahmadi Departement of Internal Medicine Sintang - 2013Документ98 страницNormal Ecg, Infarction & Arrhythmias: Iqbal Lahmadi Departement of Internal Medicine Sintang - 2013Maylisa ManurungОценок пока нет
- Ecg 4Документ18 страницEcg 4api-3757039100% (3)
- Comprehensive Board ReviewДокумент127 страницComprehensive Board Reviewlfei1216Оценок пока нет
- Acs HarkitДокумент100 страницAcs HarkittammypusphitarОценок пока нет
- CLIX ECG Tutorial Part 3 Ischaemia EtcДокумент97 страницCLIX ECG Tutorial Part 3 Ischaemia Etcdragon66Оценок пока нет
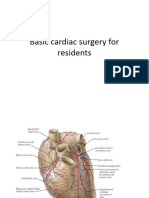
- Basic Cardiac Surgery For ResidentsДокумент53 страницыBasic Cardiac Surgery For ResidentsIntrusive ReaderОценок пока нет
- Ecginami 111115073242 Phpapp02Документ104 страницыEcginami 111115073242 Phpapp02ginaul100% (1)
- BUrvand All ABout STEMIs PDFДокумент66 страницBUrvand All ABout STEMIs PDFPryaОценок пока нет
- Interpretasi ECG Dr. SallyДокумент66 страницInterpretasi ECG Dr. SallyRichard GunawanОценок пока нет
- ECG Brief NotesДокумент5 страницECG Brief NotesKalpani Malsha UdawelagedaraОценок пока нет
- Introduction To Interpretation V10.0 (2017-2018)Документ91 страницаIntroduction To Interpretation V10.0 (2017-2018)Muhammad AsrudinОценок пока нет
- 11 Steps of ECG - Ali Alnahari PDFДокумент16 страниц11 Steps of ECG - Ali Alnahari PDFBìnhОценок пока нет
- Sirkulasi KorenerДокумент67 страницSirkulasi KorenerAmalia Frantika WihardjoОценок пока нет
- (PDF.3) Management of Heart AttackДокумент33 страницы(PDF.3) Management of Heart AttackTheany Be SmilerОценок пока нет
- Nursing Care of Patient With Cardiac ArrestДокумент78 страницNursing Care of Patient With Cardiac ArrestNurhamizah Abd hamidОценок пока нет
- ECG Patterns of Isolated RightДокумент5 страницECG Patterns of Isolated RightandreaОценок пока нет
- Premature Ventricular Contraction:: Treat It or Leave ItДокумент49 страницPremature Ventricular Contraction:: Treat It or Leave ItHanifa Bi BaritoОценок пока нет
- JCC Stemi CompleteДокумент36 страницJCC Stemi Completeb aОценок пока нет
- Cardiovascular Emergencies - EMB 2017 - DR AndriaДокумент95 страницCardiovascular Emergencies - EMB 2017 - DR AndriaJeffrey EkaОценок пока нет
- 2020.ischemic Electrocardiographic Changes and Correlation With RegionsДокумент15 страниц2020.ischemic Electrocardiographic Changes and Correlation With RegionsWeila dos Santos VieiraОценок пока нет
- Heart - PathologyДокумент22 страницыHeart - Pathologyjmosser100% (1)
- IMA Nurse KKV SaifurДокумент69 страницIMA Nurse KKV Saifureva munartyОценок пока нет
- ECG ECHO12007 NotesДокумент133 страницыECG ECHO12007 NotescassandramacphersonОценок пока нет
- CCRN-PCCN-CMC Review Cardiac Part 1 PDFДокумент14 страницCCRN-PCCN-CMC Review Cardiac Part 1 PDFGiovanni Mictil100% (1)
- ECG VCG in Left Ventricular Hypertrophy Enlargements LVH Part 1Документ57 страницECG VCG in Left Ventricular Hypertrophy Enlargements LVH Part 1Nguyen TuanОценок пока нет
- Anterior Myocardial InfarctionДокумент14 страницAnterior Myocardial InfarctionUtami HandayaniОценок пока нет
- 5.RCA or LCX in Inferior MIДокумент7 страниц5.RCA or LCX in Inferior MIAshraf ChowdhuryОценок пока нет
- Approach To Ecgs: Rhythm Check RateДокумент5 страницApproach To Ecgs: Rhythm Check RateAnanda NadaradjaneОценок пока нет
- 5 ECG Interpretation With AnswersДокумент48 страниц5 ECG Interpretation With AnswersQusai Ibraheem100% (1)
- Acute MiДокумент61 страницаAcute MiMalueth AnguiОценок пока нет
- Curs de Chirurgie Cardiaca PT StudentiДокумент86 страницCurs de Chirurgie Cardiaca PT StudentiLozan GabrielaОценок пока нет
- Basic ECG Interpretation For CoassДокумент61 страницаBasic ECG Interpretation For Coassronykharisma17Оценок пока нет
- Acute Coronary Syndromes: Acute MI and Unstable Angina: Tintinalli Chapter 50 September 20, 2005Документ62 страницыAcute Coronary Syndromes: Acute MI and Unstable Angina: Tintinalli Chapter 50 September 20, 2005Jibak MajumderОценок пока нет
- Common ECG With Management For Family Medicine ResidentsДокумент19 страницCommon ECG With Management For Family Medicine ResidentsdrhassanashrafeОценок пока нет
- Basic ECG Interpretation For CoassДокумент61 страницаBasic ECG Interpretation For CoassSlamet Katib100% (1)
- Interpreting The Athlete's ECGДокумент10 страницInterpreting The Athlete's ECGVaniaAlmiraОценок пока нет
- Basicelectrocardiogram ppt2013Документ134 страницыBasicelectrocardiogram ppt2013Catalin LeonteОценок пока нет
- A Simplified ECG GuideДокумент4 страницыA Simplified ECG Guidejalan_z96% (27)
- Tri Fascicular BlockДокумент28 страницTri Fascicular BlockSubhashini KОценок пока нет
- ECG Interpretations For MI-2020Документ10 страницECG Interpretations For MI-2020Vebot100% (1)
- Clinical ECG RoundsДокумент2 страницыClinical ECG RoundsKai Siang ChanОценок пока нет
- Diferenciacion Electrocardiografica de CX y CD en Cara InferiorДокумент8 страницDiferenciacion Electrocardiografica de CX y CD en Cara InferiorRenzo RosalesОценок пока нет
- Introduction and Objectives: ST Elevation MIДокумент7 страницIntroduction and Objectives: ST Elevation MIGio Vano NaihonamОценок пока нет
- Dr. Firman Leksmono SP - JP Basic ECG Interpretation For StudentДокумент54 страницыDr. Firman Leksmono SP - JP Basic ECG Interpretation For Studentadela_97line100% (2)
- Anatomy of The Coronary Arteries and VeinsДокумент80 страницAnatomy of The Coronary Arteries and Veinstreelife111Оценок пока нет
- Jurnal KardioДокумент3 страницыJurnal KardioSyilla PriscilliaОценок пока нет
- Tachycardia Approach and ManagementДокумент41 страницаTachycardia Approach and ManagementChadi Alraies100% (5)
- Acute Choronary SyndromeДокумент7 страницAcute Choronary SyndromeSafana NazeerОценок пока нет
- EKG+Mastery +ischemia PDFДокумент6 страницEKG+Mastery +ischemia PDFCatur Ari Intan PuspitasariОценок пока нет
- EKG+Mastery +ischemiaДокумент6 страницEKG+Mastery +ischemiamoussa medjahedОценок пока нет
- Essential Cardiac Electrophysiology: The Self-Assessment ApproachОт EverandEssential Cardiac Electrophysiology: The Self-Assessment ApproachОценок пока нет
- Tumor: Dr. Ardizal Rahman, SPMДокумент30 страницTumor: Dr. Ardizal Rahman, SPMnurul ramadhiniОценок пока нет
- Dysmenorhea: DR - Dedy Hendry, Spog-Kfer Konsultan Fertilitas Endokrin Dan ReproduksiДокумент25 страницDysmenorhea: DR - Dedy Hendry, Spog-Kfer Konsultan Fertilitas Endokrin Dan Reproduksinurul ramadhiniОценок пока нет
- Glaucoma: DR - Fitratul Ilahi, SPM (K)Документ47 страницGlaucoma: DR - Fitratul Ilahi, SPM (K)nurul ramadhiniОценок пока нет
- An Approach To Movement Disorders: Basjiruddin A Department of Neurology University of Andalas Padang 2018Документ46 страницAn Approach To Movement Disorders: Basjiruddin A Department of Neurology University of Andalas Padang 2018nurul ramadhiniОценок пока нет
- KP 2.5.4.5 AortaДокумент60 страницKP 2.5.4.5 Aortanurul ramadhiniОценок пока нет
- KP 2.5.5.3 Cor PulmonaleДокумент17 страницKP 2.5.5.3 Cor Pulmonalenurul ramadhiniОценок пока нет
- KP 2.5.5.6 115424 - Cardiac Arrest Step by StepДокумент26 страницKP 2.5.5.6 115424 - Cardiac Arrest Step by Stepnurul ramadhiniОценок пока нет
- KP 2.5.3.1 - Infektif Endokarditis (DESKTOP-Q6ABKJN's Conflicted Copy 2017-05-04)Документ125 страницKP 2.5.3.1 - Infektif Endokarditis (DESKTOP-Q6ABKJN's Conflicted Copy 2017-05-04)nurul ramadhiniОценок пока нет
- KP 2.5.5.1 Gagal Jantung KronikДокумент39 страницKP 2.5.5.1 Gagal Jantung Kroniknurul ramadhiniОценок пока нет
- KP 2.5.5.4 112027 - Shock FKGДокумент39 страницKP 2.5.5.4 112027 - Shock FKGnurul ramadhiniОценок пока нет
- K07 - Respi HIV AnakДокумент39 страницK07 - Respi HIV Anaknurul ramadhiniОценок пока нет
- Bab 39 Renjatan AnafilaktikДокумент3 страницыBab 39 Renjatan Anafilaktiknurul ramadhiniОценок пока нет
- Valvular Heart Disease: Aortic RegurgitationДокумент14 страницValvular Heart Disease: Aortic Regurgitationnurul ramadhiniОценок пока нет
- Valvular Heart Disease: Mitral StenosisДокумент23 страницыValvular Heart Disease: Mitral Stenosisnurul ramadhiniОценок пока нет
- Rad Energy System TrainДокумент8 страницRad Energy System TraincoachhandОценок пока нет
- Name: Reycel Ann L. Ilawan Section: F Reference: Puhl, R., Rubino, F., Cummings, D., Eckel, R., & Ryan, D. (2020) - Joint InternationalДокумент3 страницыName: Reycel Ann L. Ilawan Section: F Reference: Puhl, R., Rubino, F., Cummings, D., Eckel, R., & Ryan, D. (2020) - Joint InternationalReycel IlawanОценок пока нет
- Calories ChartДокумент12 страницCalories ChartRahul SharmaОценок пока нет
- Endo Main Base LvivtechДокумент103 страницыEndo Main Base LvivtechGiridhar SolasaОценок пока нет
- Pathophysiology - Diabetes Mellitus Type 2Документ3 страницыPathophysiology - Diabetes Mellitus Type 2Francis Kevin Sagudo100% (10)
- NutraHacker Complete SASДокумент9 страницNutraHacker Complete SASJustin KellyОценок пока нет
- Core Fitness Zone Resistance BandsДокумент47 страницCore Fitness Zone Resistance BandsSandesh100% (5)
- Term Paper On Heart DiseaseДокумент4 страницыTerm Paper On Heart Diseaseea9k5d7j100% (1)
- Daftar PustakaДокумент3 страницыDaftar PustakaIndri NizaОценок пока нет
- Referat Distosia Bahu ElfaДокумент16 страницReferat Distosia Bahu ElfaElfa RiniОценок пока нет
- KKKKKKKKKKKKДокумент15 страницKKKKKKKKKKKKPin Han NaОценок пока нет
- Alkaline Water: The Disease Fighting WaterДокумент9 страницAlkaline Water: The Disease Fighting WaterSaid NafikОценок пока нет
- Alcohol and PancreatitisДокумент2 страницыAlcohol and Pancreatitishrpwmv83Оценок пока нет
- Ingilizce Dil Bilgisi Ve Kelime Testleri KitabiДокумент365 страницIngilizce Dil Bilgisi Ve Kelime Testleri KitabiRuya SОценок пока нет
- Standards of Care in Diabetes - 2023Документ12 страницStandards of Care in Diabetes - 2023Menethil Terenas ElijiahОценок пока нет
- Eating Disorders LP 2013Документ28 страницEating Disorders LP 2013muscalualina100% (1)
- SGD Gross AnatomyДокумент11 страницSGD Gross Anatomyluis_chubeeОценок пока нет
- Biostatistics: A Refresher: Kevin M. Sowinski, Pharm.D., FCCPДокумент20 страницBiostatistics: A Refresher: Kevin M. Sowinski, Pharm.D., FCCPNaji Mohamed Alfatih100% (1)
- Rizal Technological University Institute of Physical EducationДокумент1 страницаRizal Technological University Institute of Physical EducationJoshua OvillaОценок пока нет
- Basic Biometrics StudentДокумент71 страницаBasic Biometrics StudentKatie100% (1)
- Six-Week Beginner Walking Plan: Monday Tuesday Wednesday Thursday Friday Weekend WorkoutДокумент1 страницаSix-Week Beginner Walking Plan: Monday Tuesday Wednesday Thursday Friday Weekend WorkoutJason SpottsОценок пока нет
- Pullups From Zero To HeroДокумент12 страницPullups From Zero To HeroBruno Heuer100% (2)
- Kefir Improves Blood Parameters and Reduces Cardiovascular Risks in Patients With Metabolic SyndromeДокумент7 страницKefir Improves Blood Parameters and Reduces Cardiovascular Risks in Patients With Metabolic SyndromeCristina OliveiraОценок пока нет
- Pathophysiology of Chronic Renal Failure PDFДокумент4 страницыPathophysiology of Chronic Renal Failure PDFDewa Made Rendy SanjayaОценок пока нет
- Energy Requirements For AdultsДокумент3 страницыEnergy Requirements For AdultsSyifa MustikaОценок пока нет
- FitCamps Timetable 2014 PDFДокумент3 страницыFitCamps Timetable 2014 PDFJasmine LoveОценок пока нет
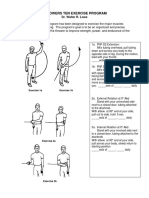
- LP 1throwers - Ten - Exercises - 2010 PDFДокумент5 страницLP 1throwers - Ten - Exercises - 2010 PDFClaudiaОценок пока нет
- Diet Therapy: Clinical NutritionДокумент7 страницDiet Therapy: Clinical NutritionLoren LacasandileОценок пока нет
- 5 Altered Nutrition Less Than Body Requirements Chronic Renal Failure Nursing Care PlansДокумент3 страницы5 Altered Nutrition Less Than Body Requirements Chronic Renal Failure Nursing Care Plansjustin_sane40% (5)
- Why Do Human Cells Rely Far More On Glucose and Fat For The Energy Than On ProteinДокумент4 страницыWhy Do Human Cells Rely Far More On Glucose and Fat For The Energy Than On ProteinHamda HassanОценок пока нет