Вам также может понравиться
- Management of Tuberculosis: A guide for clinicians (eBook edition)От EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Оценок пока нет
- Cellular AberrationsДокумент94 страницыCellular AberrationsKatherineCentenoIlaganRNОценок пока нет
- Cellular AberrationДокумент14 страницCellular AberrationjinahyangОценок пока нет
- Cellular AberrationДокумент2 страницыCellular AberrationFrances Gaviola100% (1)
- 18 Cellular AberrationsДокумент70 страниц18 Cellular AberrationsBea Bianca CruzОценок пока нет
- Cellular AberrationДокумент70 страницCellular Aberrationmatrixtrinity100% (2)
- Cellular Aberration QuizДокумент7 страницCellular Aberration QuizTherese Melchie SantuyoОценок пока нет
- D and CДокумент37 страницD and CMary Grace MasОценок пока нет
- NCM 109 2023 F-ACAD-29 - Syllabus Template (Rev 6)Документ63 страницыNCM 109 2023 F-ACAD-29 - Syllabus Template (Rev 6)Joyce EricaОценок пока нет
- NCM 112 Lecture Module 4 Cellular AberrationДокумент16 страницNCM 112 Lecture Module 4 Cellular AberrationMeryville JacildoОценок пока нет
- Community Health Nursing ReviewerДокумент24 страницыCommunity Health Nursing ReviewergilpogsОценок пока нет
- FILARIASISДокумент2 страницыFILARIASIShaoc0425Оценок пока нет
- Objectives CriticalcareДокумент2 страницыObjectives CriticalcareKharlene Mae I. Olandres100% (1)
- Intensive Nursing Practicum: Bachelor of Science in NursingДокумент9 страницIntensive Nursing Practicum: Bachelor of Science in NursingMichelle Gliselle Guinto MallareОценок пока нет
- NCM 417 Modular Exam 1Документ7 страницNCM 417 Modular Exam 1joyrena ochondraОценок пока нет
- Electrocardiogram Return Demonstration ScriptДокумент3 страницыElectrocardiogram Return Demonstration ScriptRio Dante100% (1)
- Competency Standards of Nursing Practice in The PhilippinesДокумент5 страницCompetency Standards of Nursing Practice in The Philippinespamcarl100% (2)
- A. Nursing Process in The Care of Population, Groups, and CommunityДокумент6 страницA. Nursing Process in The Care of Population, Groups, and Communityanne marie50% (2)
- NCM 114: Care of The Older Adult Instructor: Gino Paulo A. Buizon, R.NДокумент9 страницNCM 114: Care of The Older Adult Instructor: Gino Paulo A. Buizon, R.NJay VillasotoОценок пока нет
- NCP & Drugstudy FormatДокумент7 страницNCP & Drugstudy Formatanonymous89ify100% (1)
- University of San Carlos College of NursingДокумент1 страницаUniversity of San Carlos College of NursingfabaquitaОценок пока нет
- Care of Clients With Problems in Cellular AberrationДокумент50 страницCare of Clients With Problems in Cellular AberrationNina Anne Paracad100% (3)
- 12 Health Indicator LegendsДокумент4 страницы12 Health Indicator LegendsEmman TeewaiОценок пока нет
- Disaster Preparedness - Leadership and Coordination in Disaster in Health Care System With LectureДокумент29 страницDisaster Preparedness - Leadership and Coordination in Disaster in Health Care System With LectureArvie ReyesОценок пока нет
- Oncology Nursing Handouts 1Документ8 страницOncology Nursing Handouts 1pauchanmnlОценок пока нет
- CRMC Medication TicketsДокумент2 страницыCRMC Medication TicketsMarielle Chua100% (1)
- Philippine Health Agenda - Dec1 - 1 PDFДокумент26 страницPhilippine Health Agenda - Dec1 - 1 PDFreyalene gallegosОценок пока нет
- NCM 121 FinalsДокумент8 страницNCM 121 FinalsKhen QuiringОценок пока нет
- Lesson 1 - Intro To Nursing Research 1Документ24 страницыLesson 1 - Intro To Nursing Research 1Jaylen CayОценок пока нет
- Ethico-Moral Principles and Cultural/Spiritual Preferences: By: Kim Angelique TinoДокумент14 страницEthico-Moral Principles and Cultural/Spiritual Preferences: By: Kim Angelique TinoPRIMA, CAMILLE JOY ROSELAОценок пока нет
- Pre Test Rle70.medical Ward NMMC Cagayan de Oro CityДокумент6 страницPre Test Rle70.medical Ward NMMC Cagayan de Oro CityLouresa Mae TОценок пока нет
- DM and Oncology Semi Finals QuizДокумент15 страницDM and Oncology Semi Finals QuizKaren mae alvarroОценок пока нет
- Blood Pressure Measurement Is An Important Part of The Patient's Data Base. It Is Considered To BeДокумент1 страницаBlood Pressure Measurement Is An Important Part of The Patient's Data Base. It Is Considered To BeMir MirОценок пока нет
- Nursing Care Plan: Subjective Data " GoalДокумент2 страницыNursing Care Plan: Subjective Data " GoalJay VillasotoОценок пока нет
- Chickenpox 1Документ7 страницChickenpox 1Nica Joy CandelarioОценок пока нет
- Predisposing Factor Disease Process Signs and Symptoms Medications Medical Interventions Medical DiagnosisДокумент4 страницыPredisposing Factor Disease Process Signs and Symptoms Medications Medical Interventions Medical DiagnosisSkyla FiestaОценок пока нет
- Nursing Care Plan For Breast Cancer NCP PDFДокумент2 страницыNursing Care Plan For Breast Cancer NCP PDFMaina BarmanОценок пока нет
- Health Care Delivery System & COPARДокумент52 страницыHealth Care Delivery System & COPARDharylle Cariño100% (1)
- Nursing Associations in The PhilippinesДокумент18 страницNursing Associations in The PhilippinesGumama AmeiyrhaОценок пока нет
- Cellular Aberrations Cancer, Malignant Neoplasm, Oncologic DisorderДокумент5 страницCellular Aberrations Cancer, Malignant Neoplasm, Oncologic DisorderIrish Eunice Felix100% (1)
- Pscy PrelimДокумент20 страницPscy PrelimAinah Batua-anОценок пока нет
- Computer Generated in Nursing Care PlansДокумент4 страницыComputer Generated in Nursing Care PlansCake Man100% (1)
- Cell Ab ActivitiesДокумент7 страницCell Ab ActivitiesJanelle Cabida Supnad100% (1)
- No. 10 SANAANI Topic For Esophagogastric Balloon Tamponade Tubes Billroth 1 and 11Документ12 страницNo. 10 SANAANI Topic For Esophagogastric Balloon Tamponade Tubes Billroth 1 and 11Nur SanaaniОценок пока нет
- Ra 9288 (NBS)Документ6 страницRa 9288 (NBS)John Paul SibayanОценок пока нет
- TFN SyllabusДокумент1 страницаTFN SyllabusVincent Quiña PigaОценок пока нет
- Balance Skeletal TractionДокумент5 страницBalance Skeletal TractionRachel Ann JimenezОценок пока нет
- Legal Psychiatric Nursing Issues Commitment IssuesДокумент17 страницLegal Psychiatric Nursing Issues Commitment IssuesBrandon Arete100% (1)
- Predisposing Factors Age Diet Dehydration Precipitating Factors Family or Personal History Digestive Diseases and SurgeryДокумент2 страницыPredisposing Factors Age Diet Dehydration Precipitating Factors Family or Personal History Digestive Diseases and SurgeryChloé Jane HilarioОценок пока нет
- The Nursing Diagnosis Body Image Disturbance Is Most Likely To Be Written For Which of The Following PersonsДокумент3 страницыThe Nursing Diagnosis Body Image Disturbance Is Most Likely To Be Written For Which of The Following PersonsenzoОценок пока нет
- Transcultural Nursing QuizДокумент3 страницыTranscultural Nursing QuizBelle A. BasilioОценок пока нет
- (DOH Programs) A. Expanded Program On Immunization: Legal BasisДокумент90 страниц(DOH Programs) A. Expanded Program On Immunization: Legal BasisRichard Deo R. AlaveОценок пока нет
- Nursing Associations in The PhilippinesДокумент10 страницNursing Associations in The PhilippinesShara SampangОценок пока нет
- Cellular AberrationДокумент58 страницCellular AberrationTauqeer AhmedОценок пока нет
- Prepared By: Anna Marie M. Montalban, RN, Us-RnДокумент71 страницаPrepared By: Anna Marie M. Montalban, RN, Us-RnPrecai Permangil100% (2)
- Oncology NursingДокумент7 страницOncology NursingDiana Laura Lei100% (1)
- Is Module 8Документ26 страницIs Module 8gladyskheyagamОценок пока нет
- NE0PLASIAДокумент28 страницNE0PLASIADaniel SutantoОценок пока нет
- Chapter 6 NeoplasiaДокумент24 страницыChapter 6 Neoplasiahenna patelОценок пока нет
- Name: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicДокумент8 страницName: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicAnoosha FarooquiОценок пока нет
- PCM (8) Test For Significance (Dr. Tante)Документ151 страницаPCM (8) Test For Significance (Dr. Tante)Kris TejereroОценок пока нет
- Histology RespiДокумент4 страницыHistology RespiKris TejereroОценок пока нет
- Ronel NaireДокумент4 страницыRonel NaireKris TejereroОценок пока нет
- Dr. Edgar Gasco Anatomy LabДокумент3 страницыDr. Edgar Gasco Anatomy LabKris TejereroОценок пока нет
- Lab ANA Set 2Документ6 страницLab ANA Set 2Kris TejereroОценок пока нет
- School Stage RoofingДокумент12 страницSchool Stage RoofingKris TejereroОценок пока нет
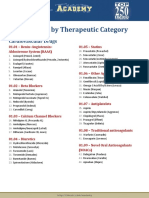
- Drug List by Therapeutic Category: Cardiovascular DrugsДокумент7 страницDrug List by Therapeutic Category: Cardiovascular DrugsAloah122346Оценок пока нет
- Vaccine Minimum Age at 1st Dose Number of Doses Dose Minimum Interval Between Doses Route Site ReasonДокумент4 страницыVaccine Minimum Age at 1st Dose Number of Doses Dose Minimum Interval Between Doses Route Site ReasonKris TejereroОценок пока нет
- NCM 104 Cellular Aberration Lecture 2007Документ104 страницыNCM 104 Cellular Aberration Lecture 2007Kris TejereroОценок пока нет
- By: Kris Lyn L. TejereoДокумент30 страницBy: Kris Lyn L. TejereoKris TejereroОценок пока нет
- Nursing Care Plan: Name of Patient: - Age: - SexДокумент4 страницыNursing Care Plan: Name of Patient: - Age: - SexKris TejereroОценок пока нет
- Pharma Reviewer From VinnyДокумент16 страницPharma Reviewer From VinnyKris TejereroОценок пока нет
- Area Inspection Palpation Auscultation Percussion: Physical AssessmentДокумент6 страницArea Inspection Palpation Auscultation Percussion: Physical AssessmentKris TejereroОценок пока нет
- Algor Mortis - Cooling of The Body-: Antemortem Agonal Period Postmortem Postmortem ChangesДокумент13 страницAlgor Mortis - Cooling of The Body-: Antemortem Agonal Period Postmortem Postmortem ChangesKris TejereroОценок пока нет
- Laboratory Studies: FecalysisДокумент2 страницыLaboratory Studies: FecalysisKris TejereroОценок пока нет
- HIV DrugsДокумент31 страницаHIV DrugsKris TejereroОценок пока нет
- Process Recording WMCCДокумент3 страницыProcess Recording WMCCKris TejereroОценок пока нет
- Rheumatic Fever PDFДокумент3 страницыRheumatic Fever PDFDoc JT BylnОценок пока нет
- Contact Lens Complications and ManagementДокумент10 страницContact Lens Complications and Managementstrawberry8832850% (2)
- Pharmaceutical Market Europe - June 2020Документ50 страницPharmaceutical Market Europe - June 2020Areg GhazaryanОценок пока нет
- Clinical Microbiology and Infection: Original ArticleДокумент6 страницClinical Microbiology and Infection: Original ArticleAkira Masumi100% (1)
- Principles of Adolescent Substance Use Disorder Treatment PDFДокумент42 страницыPrinciples of Adolescent Substance Use Disorder Treatment PDFDanilo CozzoliОценок пока нет
- Second Hand Smoke Fact SheetДокумент9 страницSecond Hand Smoke Fact Sheetwesa77Оценок пока нет
- HTTP Oyc - Yale.edu Yale Psychology Introduction-To-psychology Content Transcripts Transcript 11Документ7 страницHTTP Oyc - Yale.edu Yale Psychology Introduction-To-psychology Content Transcripts Transcript 11Amol ShashiОценок пока нет
- Lesson Plan Renal CalculiДокумент17 страницLesson Plan Renal CalculiAmrita Dean71% (7)
- Hosa Happenings 2021 1Документ8 страницHosa Happenings 2021 1api-524471148Оценок пока нет
- Psychoactive Drugs ChartДокумент5 страницPsychoactive Drugs ChartAlessandra WilliamsОценок пока нет
- USMLE Step 1 First Aid 2021-101-230Документ130 страницUSMLE Step 1 First Aid 2021-101-230mariana yllanesОценок пока нет
- ST Peter, 2014, BI-Annual DR-TB Performance Report To AAHB, 15 March 2022. JohnДокумент43 страницыST Peter, 2014, BI-Annual DR-TB Performance Report To AAHB, 15 March 2022. Johnሀይደር ዶ.ርОценок пока нет
- 110 ch3Документ3 страницы110 ch3Hitesh KhuranaОценок пока нет
- Case Study Presentation-Mindy Duran-FinalДокумент30 страницCase Study Presentation-Mindy Duran-Finalapi-278622211Оценок пока нет
- WelcomeДокумент74 страницыWelcomeSagarRathodОценок пока нет
- Bite Force and Occlusion-Merete Bakke 2006Документ7 страницBite Force and Occlusion-Merete Bakke 2006Dan MPОценок пока нет
- Rizal in DapitanДокумент2 страницыRizal in DapitanMary Nicole PaedОценок пока нет
- Splice PDFДокумент5 страницSplice PDFpedroОценок пока нет
- Burdens of Family Caregiving at The End of LifeДокумент6 страницBurdens of Family Caregiving at The End of LifeNurul ShahirahОценок пока нет
- Stress Management Strategies Adopted by Teachers in Public Primary Schools in Obio/Akpor Local Government Area of Rivers State, Nigeria.Документ94 страницыStress Management Strategies Adopted by Teachers in Public Primary Schools in Obio/Akpor Local Government Area of Rivers State, Nigeria.sorbariОценок пока нет
- John Medina - Brain Rules PDFДокумент11 страницJohn Medina - Brain Rules PDFDiego Cunha100% (2)
- Maret 18 PDFДокумент178 страницMaret 18 PDFAnonymous vLgCd0U7Оценок пока нет
- US - Inggris 2017Документ5 страницUS - Inggris 2017SmabaitulhikmahОценок пока нет
- Brain Biochemistry and DisordersДокумент191 страницаBrain Biochemistry and DisordersTrajce PasowskyОценок пока нет
- Yoga Poses For Acid RefluxДокумент6 страницYoga Poses For Acid RefluxKirit JhaОценок пока нет
- Diagnostic TestДокумент4 страницыDiagnostic TestrizabesmonteОценок пока нет
- Feed Additives, Antibodies, Poultry Vaccines 2023.3Документ6 страницFeed Additives, Antibodies, Poultry Vaccines 2023.3Bruce YangОценок пока нет
- Theory ApplicationДокумент38 страницTheory ApplicationAnusha VergheseОценок пока нет
- Bats MagicДокумент5 страницBats MagicANDROMEDA1974Оценок пока нет
- HRCT in Diffuse Lung Diseases - II: Dr. Bhavin JankhariaДокумент33 страницыHRCT in Diffuse Lung Diseases - II: Dr. Bhavin JankhariaAbdul QuyyumОценок пока нет