Вам также может понравиться
- Medical Encyclopedia XXL: Prof. J.P. Schadé, M.D., Ph.D. D.Sc.hcОт EverandMedical Encyclopedia XXL: Prof. J.P. Schadé, M.D., Ph.D. D.Sc.hcОценок пока нет
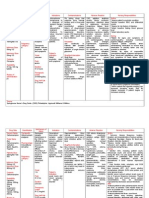
- Receptor Profile of Selected Anti-Psychotic Drugs: Lovely Liana Clapis Sittie Rahani CanacanДокумент42 страницыReceptor Profile of Selected Anti-Psychotic Drugs: Lovely Liana Clapis Sittie Rahani CanacanKevin ChanОценок пока нет
- Antipsychotics: Mechanisms and Clinical UsesДокумент47 страницAntipsychotics: Mechanisms and Clinical UsesSharah Stephanie IIОценок пока нет
- PA 644 - M2 LecturesДокумент735 страницPA 644 - M2 LectureskatОценок пока нет
- PA 644 - M2 LecturesДокумент412 страницPA 644 - M2 LectureskatОценок пока нет
- Understanding Antipsychotics: Uses, Side Effects & ClassificationДокумент26 страницUnderstanding Antipsychotics: Uses, Side Effects & ClassificationtemitopeОценок пока нет
- Biological Treatments in PsychiatryДокумент56 страницBiological Treatments in PsychiatryNurul AfzaОценок пока нет
- Drug Study Mother TДокумент14 страницDrug Study Mother TEuzelle Jeena ArandaОценок пока нет
- Second Generation AntipsychoticsДокумент58 страницSecond Generation AntipsychoticsUBONGABASI EYO100% (1)
- AntipsychoticsДокумент58 страницAntipsychoticsnithin shenoiОценок пока нет
- ClonazepamДокумент3 страницыClonazepamapi-3797941Оценок пока нет
- Treatment For Mental Health IssuesДокумент43 страницыTreatment For Mental Health Issuessang Nguyen DuongОценок пока нет
- PsychopharmacologyДокумент50 страницPsychopharmacologyapi-3703352Оценок пока нет
- AntipsychoticsДокумент36 страницAntipsychoticsGlory MimiОценок пока нет
- Drug StudyДокумент11 страницDrug StudyJohn LesterОценок пока нет
- BPAD FinalДокумент31 страницаBPAD FinalZAОценок пока нет
- AlprazolamДокумент3 страницыAlprazolamapi-3797941100% (1)
- Antipsychotics 44Документ65 страницAntipsychotics 44bemnetОценок пока нет
- Drug StudyДокумент12 страницDrug StudyAngeli A EstilloreОценок пока нет
- Drugs Used in Mental IllnessДокумент60 страницDrugs Used in Mental IllnessDixa MeОценок пока нет
- Anti Psych TicsДокумент44 страницыAnti Psych TicshamzabhayatОценок пока нет
- Antiparkinsonian DrugsДокумент35 страницAntiparkinsonian DrugsvimalaОценок пока нет
- Chlorpromazine for schizophrenia and nauseaДокумент6 страницChlorpromazine for schizophrenia and nauseaAnonymous cwlpSlReUYОценок пока нет
- Risperidone Guide: Uses, Dosage, Side EffectsДокумент9 страницRisperidone Guide: Uses, Dosage, Side EffectsChresia Schae MondejarОценок пока нет
- Antipsychotic Drugs - Wafa Bin ShamlanДокумент8 страницAntipsychotic Drugs - Wafa Bin ShamlanSara AbdoОценок пока нет
- Anti Psychotic DrugДокумент25 страницAnti Psychotic DrugANI SAMОценок пока нет
- Second Gen AtipsychoticДокумент34 страницыSecond Gen Atipsychoticemamma hashirОценок пока нет
- Antipsychotic Drugs: Reported by Rex MendozaДокумент19 страницAntipsychotic Drugs: Reported by Rex MendozaKate NavarroОценок пока нет
- Module 8Документ5 страницModule 8Yuki Xairah TunayОценок пока нет
- Drug Induced Movement DisordersДокумент65 страницDrug Induced Movement DisordersShaunak PatilОценок пока нет
- Parkinson's Disease Review of Pathophysiology, Diagnosis and Current TherapyДокумент38 страницParkinson's Disease Review of Pathophysiology, Diagnosis and Current TherapyYurissa KarimahОценок пока нет
- DRUGS FOR PARKINSON'S DISEASE AND MIGRAINEДокумент49 страницDRUGS FOR PARKINSON'S DISEASE AND MIGRAINEGarry SoloanОценок пока нет
- Olanzapine Nursing Care GuideДокумент3 страницыOlanzapine Nursing Care GuideBarbara Detaro100% (2)
- Pharmacological Management of DepressionДокумент66 страницPharmacological Management of DepressionPriyash JainОценок пока нет
- Drug StudyДокумент10 страницDrug StudyRubie Ann TillorОценок пока нет
- 5-Drugs Used in Parkinsonism Summary and QuestionsДокумент7 страниц5-Drugs Used in Parkinsonism Summary and QuestionsmugtabaОценок пока нет
- 3.3.4.4 DRUG in PSYCHIATRIC DISORDERДокумент31 страница3.3.4.4 DRUG in PSYCHIATRIC DISORDERyunielsyaОценок пока нет
- LithiumДокумент4 страницыLithiumapi-3797941100% (1)
- Drug-Induced Movement Disorders GuideДокумент136 страницDrug-Induced Movement Disorders GuideYamini DevendranОценок пока нет
- Drug Presentation: Manisha M.Sc. Nursing 1 Year Con IlbsДокумент57 страницDrug Presentation: Manisha M.Sc. Nursing 1 Year Con IlbsManisha ShakyaОценок пока нет
- Understanding Monoamine Hypothesis of DepressionДокумент58 страницUnderstanding Monoamine Hypothesis of Depressionrayinda mamahitОценок пока нет
- Antipsychotic DrugsДокумент3 страницыAntipsychotic DrugsArtt1975Оценок пока нет
- Antipsychotics Risks and BenefitsДокумент38 страницAntipsychotics Risks and BenefitsElleОценок пока нет
- Drug StudyДокумент106 страницDrug StudyBlessie Mae Guinanghan AbuanОценок пока нет
- Risperidone: An Atypical AntipsychoticДокумент16 страницRisperidone: An Atypical Antipsychoticshreshta reddy PalleОценок пока нет
- Pharmacogenomics Guide Genetic Variation Drug ResponseДокумент22 страницыPharmacogenomics Guide Genetic Variation Drug ResponseLalit GuptaОценок пока нет
- Archivetempfinal RevisionДокумент140 страницArchivetempfinal RevisionSheza FarooqОценок пока нет
- BPJ 40 Antipsychotics Pages 14-23Документ10 страницBPJ 40 Antipsychotics Pages 14-23James BondОценок пока нет
- Mood Disorders StudentДокумент32 страницыMood Disorders StudentRafly FernandaОценок пока нет
- AntiepilepticsДокумент25 страницAntiepilepticsMurali Krishna Kumar MuthyalaОценок пока нет
- Table 20.2-7 Medications For Treating Alcohol DependenceДокумент1 страницаTable 20.2-7 Medications For Treating Alcohol DependenceAbdualaziz AlmalkiОценок пока нет
- Drug StudyДокумент10 страницDrug Studyrubie ann tillorОценок пока нет
- Stage 1 Seminar: Clinical Pharmacology of The Nervous SystemДокумент38 страницStage 1 Seminar: Clinical Pharmacology of The Nervous SystemCollin FreemanОценок пока нет
- Drug Therapy of Schizophrenia: Applied Therapeutics IIДокумент20 страницDrug Therapy of Schizophrenia: Applied Therapeutics IIJalal AlbadriОценок пока нет
- Anti Hypertensive DrugsДокумент113 страницAnti Hypertensive DrugsRobert DowneyОценок пока нет
- Clinical Medications WorksheetsДокумент3 страницыClinical Medications WorksheetsVinz OñoОценок пока нет
- LMR Pharmacology - CnsДокумент6 страницLMR Pharmacology - CnsYuku BabyОценок пока нет
- Drug Study (Haloperidol)Документ3 страницыDrug Study (Haloperidol)Mae Ann Bueno CastillonОценок пока нет
- Pharmacology Reporting-1Документ32 страницыPharmacology Reporting-1Mj TalentОценок пока нет
- Drug AnalysisДокумент3 страницыDrug Analysiskristel_nicole18yahoОценок пока нет
- Rheumatoid Arthritis Rheumatoid Arthritis OverviewДокумент10 страницRheumatoid Arthritis Rheumatoid Arthritis OverviewayunisallehОценок пока нет
- Gyn InfertilityДокумент51 страницаGyn Infertilityayunisalleh100% (1)
- COPDДокумент6 страницCOPDayunisallehОценок пока нет
- SBA Orthopaedics (OrthoBullets) Pediatric Orthopaedics TopicsДокумент168 страницSBA Orthopaedics (OrthoBullets) Pediatric Orthopaedics Topicsayunisalleh88% (8)
- ClassificationSeizures 2017 SchefferДокумент39 страницClassificationSeizures 2017 SchefferMedstudent JombloОценок пока нет
- Personal Hygiene at TADIKUMДокумент1 страницаPersonal Hygiene at TADIKUMayunisallehОценок пока нет
- Gyn Infertility PDFДокумент8 страницGyn Infertility PDFayunisallehОценок пока нет
- Menopause (O&G)Документ19 страницMenopause (O&G)ayunisallehОценок пока нет
- The Applied Knowledge Test Content GuideДокумент51 страницаThe Applied Knowledge Test Content GuidekaralilyОценок пока нет
- Content Guide August 2013Документ54 страницыContent Guide August 2013ayunisallehОценок пока нет
- COPDДокумент6 страницCOPDayunisallehОценок пока нет
- Leukemia Long Case - NotesДокумент6 страницLeukemia Long Case - NotesayunisallehОценок пока нет
- Indian Female's Abdominal Pain and BreathlessnessДокумент12 страницIndian Female's Abdominal Pain and BreathlessnessayunisallehОценок пока нет
- CBL 2 - Case 1Документ9 страницCBL 2 - Case 1ayunisallehОценок пока нет
- RenalДокумент11 страницRenalayunisallehОценок пока нет
- Community Engagement in Public HealthДокумент5 страницCommunity Engagement in Public HealthayunisallehОценок пока нет
- Paediatrics Epileptiform DisordersДокумент11 страницPaediatrics Epileptiform DisordersayunisallehОценок пока нет
- Paediatric Diarrhoea - Lee Way SeahДокумент42 страницыPaediatric Diarrhoea - Lee Way SeahayunisallehОценок пока нет
- Newborn ScreeningДокумент46 страницNewborn ScreeningayunisallehОценок пока нет
- Central HypotoniaДокумент5 страницCentral HypotoniaayunisallehОценок пока нет
- An Approach To A Floppy InfantДокумент33 страницыAn Approach To A Floppy InfantayunisallehОценок пока нет
- Nutrition and Feeding For Infant and Young ChildrenДокумент44 страницыNutrition and Feeding For Infant and Young ChildrenayunisallehОценок пока нет
- Common Neonatal Conditions - Supplementary MaterialДокумент25 страницCommon Neonatal Conditions - Supplementary MaterialayunisallehОценок пока нет
- Crs - Neck LumpДокумент7 страницCrs - Neck LumpayunisallehОценок пока нет
- The Short ChildДокумент28 страницThe Short ChildayunisallehОценок пока нет
- Evaluation & Management of Dengue: Case StudyДокумент36 страницEvaluation & Management of Dengue: Case StudyayunisallehОценок пока нет
- Adhd and AutismДокумент50 страницAdhd and AutismayunisallehОценок пока нет
- Child at Risk Nov 2016Документ16 страницChild at Risk Nov 2016ayuniОценок пока нет
- Protocol For Deference Karen Overall 2012Документ15 страницProtocol For Deference Karen Overall 2012Sean Carlo CastilloОценок пока нет
- Drug Interactions ExplainedДокумент64 страницыDrug Interactions Explainedkaye agustinОценок пока нет
- TRINTELLIX Product Monograph EnglishДокумент45 страницTRINTELLIX Product Monograph EnglishEstmar ValentinoОценок пока нет
- Overview:: 'The Organic Chem Lab Survival Manual'Документ29 страницOverview:: 'The Organic Chem Lab Survival Manual'Jeremy Jankowski83% (6)
- Friedlander Depression 2001Документ10 страницFriedlander Depression 2001Carol LlanosОценок пока нет
- Drugs For Parkinson's Disease: Pharmacist'S Letter / Prescriber'S LetterДокумент4 страницыDrugs For Parkinson's Disease: Pharmacist'S Letter / Prescriber'S Letteranon_84599888Оценок пока нет
- Pharma (Done)Документ19 страницPharma (Done)YelОценок пока нет
- Pharmacology Review of Neuro Drugs: Antidepressants and Psychomotor StimulantsДокумент7 страницPharmacology Review of Neuro Drugs: Antidepressants and Psychomotor StimulantsDavid Hosam100% (1)
- Algesia: 37.5 MG / 325 MG Film-Coated TABLET AnalgesicДокумент1 страницаAlgesia: 37.5 MG / 325 MG Film-Coated TABLET AnalgesicEsel WazowskiОценок пока нет
- Trudy Scott Amino-AcidsДокумент35 страницTrudy Scott Amino-AcidsPreeti100% (5)
- D BL Promethazine Hydrochloride in JДокумент10 страницD BL Promethazine Hydrochloride in JarthurbaidoodouglasОценок пока нет
- ChlorpheniramineДокумент6 страницChlorpheniramineÇhämäñ ÇhОценок пока нет
- Social Anxiety DisorderДокумент10 страницSocial Anxiety DisorderLintang SuroyaОценок пока нет
- The Interaction of Herbs and DrugsДокумент17 страницThe Interaction of Herbs and DrugsCarleta StanОценок пока нет
- Joseph P. Goldberg & Carrie L. Ernst & Stephen M. Stahl - Managing The Side Effects of Psychotropic Medications-American Psychiatric Publishing (2012) PDFДокумент533 страницыJoseph P. Goldberg & Carrie L. Ernst & Stephen M. Stahl - Managing The Side Effects of Psychotropic Medications-American Psychiatric Publishing (2012) PDFbabyjesus1100% (3)
- Chapter 022 QuestionsДокумент24 страницыChapter 022 QuestionsPrecilou CutandaОценок пока нет
- Farmacoterapia en ObesidadДокумент29 страницFarmacoterapia en ObesidadAnali Durán CorderoОценок пока нет
- Imbalanced Neurotransmitters and Abnormal BehaviorДокумент3 страницыImbalanced Neurotransmitters and Abnormal BehaviorInah100% (1)
- 01 A History of The Pharmaceutical IndustryДокумент8 страниц01 A History of The Pharmaceutical IndustryHayat NaqviОценок пока нет
- Lisdexamfetamine Dimesylate - 20mg CapsuleДокумент16 страницLisdexamfetamine Dimesylate - 20mg CapsuleMd. Abdur RahmanОценок пока нет
- Poisoning - Environmental Exposure (Medicalstudyzone - Com)Документ95 страницPoisoning - Environmental Exposure (Medicalstudyzone - Com)Roshan MevadaОценок пока нет
- MIMS Abbreviation IndexДокумент1 страницаMIMS Abbreviation IndexBrian Harris100% (1)
- Mechanism and Side Effects of SSRI 1Документ13 страницMechanism and Side Effects of SSRI 1Andika MetrisiawanОценок пока нет
- Autacoids and their Antagonists ChapterДокумент37 страницAutacoids and their Antagonists ChapterJayaОценок пока нет
- UWorld NCLEX Drug ListДокумент16 страницUWorld NCLEX Drug ListAngie Mandeoya91% (11)
- CBT REVIEW MANUAL - Source Royal Marsden Clinical Nursing Procedures - Part 1Документ14 страницCBT REVIEW MANUAL - Source Royal Marsden Clinical Nursing Procedures - Part 1Lip Stick88% (32)
- Master List of Common Medical AbbreviationsДокумент37 страницMaster List of Common Medical AbbreviationshealerharishОценок пока нет
- Hypericum and DepressionДокумент38 страницHypericum and DepressionPramod SwamiОценок пока нет
- Atomoxetine LeafletДокумент2 страницыAtomoxetine LeafletFaheem khanОценок пока нет
- Food and Drug Interactions: Understanding How Nutrients Can Impact MedicationsДокумент8 страницFood and Drug Interactions: Understanding How Nutrients Can Impact MedicationsUpik MoritaОценок пока нет