Вам также может понравиться
- Parasite Identification Slides v2.0Документ25 страницParasite Identification Slides v2.0Sam Petruda100% (3)
- Nematodes NotesДокумент9 страницNematodes NotesAlbert AlegreОценок пока нет
- ATS - Contextual Theology SyllabusДокумент4 страницыATS - Contextual Theology SyllabusAts ConnectОценок пока нет
- Sakolsky Ron Seizing AirwavesДокумент219 страницSakolsky Ron Seizing AirwavesPalin WonОценок пока нет
- Enterobius VermicularisДокумент3 страницыEnterobius Vermicularisshahidkhan 654321654321Оценок пока нет
- Class Nematoda - The Roundworms Characteristics and Life CyclesДокумент76 страницClass Nematoda - The Roundworms Characteristics and Life CyclesLyraОценок пока нет
- Pin Worm Infection: Symptoms, Diagnosis and TreatmentДокумент13 страницPin Worm Infection: Symptoms, Diagnosis and Treatmentبلسم محمود شاكرОценок пока нет
- Medical Biology 6Документ58 страницMedical Biology 6Yusuf Yağız TimurОценок пока нет
- Enterobius Vermicularis - 2023Документ17 страницEnterobius Vermicularis - 2023kakukohillary48Оценок пока нет
- Strongyloides StercoralisДокумент30 страницStrongyloides StercoralisEllagEsz100% (1)
- Enterobius Vermicularis) : Hawri H. Mohammed H.D., M.Sc. ParasitologyДокумент9 страницEnterobius Vermicularis) : Hawri H. Mohammed H.D., M.Sc. ParasitologyHawre NajmaddinОценок пока нет
- Strongyloidiasis 2014Документ33 страницыStrongyloidiasis 2014officialmwalusambaОценок пока нет
- Parasit Nematodes Summer 2012Документ57 страницParasit Nematodes Summer 2012Ilham SuryoОценок пока нет
- Parasaitology HelminthДокумент139 страницParasaitology Helminthkidus asnОценок пока нет
- General Parasitology L3Документ13 страницGeneral Parasitology L3kayse abtidoonОценок пока нет
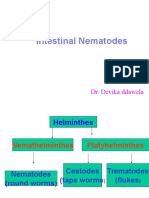
- Intestinal Nematodes: Dr. Devika DdawelaДокумент127 страницIntestinal Nematodes: Dr. Devika DdawelaPraveenKumarОценок пока нет
- Enterobius VermicularisДокумент16 страницEnterobius VermicularisYA MAAPОценок пока нет
- Aljas&Bama (Microbm9evaluate)Документ8 страницAljas&Bama (Microbm9evaluate)Mary Clare Fuentes BamaОценок пока нет
- Roun WormsДокумент24 страницыRoun WormsBalach JanОценок пока нет
- Roundworms ExplainedДокумент81 страницаRoundworms ExplainedAudrie Allyson GabalesОценок пока нет
- Revision: Types of Life Cycle in Trematoda and CestodaДокумент71 страницаRevision: Types of Life Cycle in Trematoda and CestodaMicroscopeGeekОценок пока нет
- Phylum Nematoda RoundwormsДокумент22 страницыPhylum Nematoda Roundwormserica williamsОценок пока нет
- MICROPARA-LAB-G6-Enterobius-VermicularisДокумент3 страницыMICROPARA-LAB-G6-Enterobius-VermicularisMary Jane TiangsonОценок пока нет
- EnterobiusДокумент11 страницEnterobiusMayuri VohraОценок пока нет
- Hymenolepis Nana Group 5 Write UpДокумент7 страницHymenolepis Nana Group 5 Write UpSusan GachukiaОценок пока нет
- AscarisДокумент42 страницыAscarisمصطفي خندقاوي100% (1)
- Clinical Manifestation of AscariasisДокумент28 страницClinical Manifestation of AscariasisAishah Shalimar PutriОценок пока нет
- NematodaДокумент96 страницNematodaPurplesmilezОценок пока нет
- Project IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Документ36 страницProject IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Catherine MetraОценок пока нет
- Ascaris Lumbricoides: I. MorphologyДокумент6 страницAscaris Lumbricoides: I. MorphologyJoseline SorianoОценок пока нет
- Lecture 6 2023Документ16 страницLecture 6 2023ayaessam392002Оценок пока нет
- AscarisДокумент43 страницыAscarisALBINUS AmbroseОценок пока нет
- AscariasisДокумент50 страницAscariasisAnaleah MalayaoОценок пока нет
- Ascaris LumbricoidesДокумент33 страницыAscaris LumbricoidesRosi Gustina100% (5)
- Lesson 10Документ6 страницLesson 10daryl jan komowangОценок пока нет
- E VermicularisДокумент18 страницE VermicularisYashoda AmarasekeraОценок пока нет
- N M To Es: Dr. Wafaa Ezz ElarabДокумент31 страницаN M To Es: Dr. Wafaa Ezz Elarabshoroq zaki100% (1)
- 12 - NematodaДокумент44 страницы12 - NematodaAnnisya MaharaniОценок пока нет
- Enterobius vermicularis ReportДокумент19 страницEnterobius vermicularis ReportRogelio Blanco Jr.Оценок пока нет
- Ascaris Lumbricoides: Ascariasis. Infections Most Often Seen in Young Children byДокумент7 страницAscaris Lumbricoides: Ascariasis. Infections Most Often Seen in Young Children byThea GonzalesОценок пока нет
- HYMENOLEPSIS-NANA-LABДокумент3 страницыHYMENOLEPSIS-NANA-LABMary Jane TiangsonОценок пока нет
- Nematode Infections 2019 Student PDFДокумент272 страницыNematode Infections 2019 Student PDFCharlene SuliganОценок пока нет
- Phylum NematodaДокумент24 страницыPhylum NematodaKaten KyoukotsuОценок пока нет
- Intestinal ParasitesДокумент72 страницыIntestinal ParasitesivaОценок пока нет
- MP 11 Cestodes NewДокумент46 страницMP 11 Cestodes NewGenelyn Marquez100% (1)
- AscarisДокумент3 страницыAscarisColette BarrometroОценок пока нет
- Unit - Three: HelminthsДокумент177 страницUnit - Three: HelminthsDembalu NuguseОценок пока нет
- Necator Americanus: The American Killer HookwormДокумент31 страницаNecator Americanus: The American Killer HookwormAlejandroОценок пока нет
- Para-Lab Practicals PDFДокумент15 страницPara-Lab Practicals PDFRizzy VillanuevaОценок пока нет
- Common Helminthic Infections: Symptoms, Life Cycles and TreatmentДокумент63 страницыCommon Helminthic Infections: Symptoms, Life Cycles and TreatmentRafif AmirОценок пока нет
- PARASITOLOGYДокумент57 страницPARASITOLOGYChellie GualbertoОценок пока нет
- STH's Unholy TrinityДокумент9 страницSTH's Unholy TrinityEunice AndradeОценок пока нет
- Nematodes 10-11Документ128 страницNematodes 10-11microperadeniya100% (4)
- Project IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Документ38 страницProject IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Catherine MetraОценок пока нет
- Liver flukes: Classification, morphology, life cycle, and clinical featuresДокумент31 страницаLiver flukes: Classification, morphology, life cycle, and clinical featuresحسین جاسم ستارОценок пока нет
- Case Study: MicrobiologyДокумент13 страницCase Study: MicrobiologywellYONGОценок пока нет
- THE HELMINTHS: KEY PARASITIC WORMSДокумент9 страницTHE HELMINTHS: KEY PARASITIC WORMSMomo ShinОценок пока нет
- Presentation on Ascaris Life Cycle and TreatmentДокумент13 страницPresentation on Ascaris Life Cycle and TreatmentRajanikanta MahatoОценок пока нет
- LESSON 10 Intestinal ParasitesДокумент17 страницLESSON 10 Intestinal Parasitesgimel tenorioОценок пока нет
- Ascaris LumbricoidesДокумент33 страницыAscaris LumbricoidesBio SciencesОценок пока нет
- Ancy Lost OmaДокумент41 страницаAncy Lost OmaMuhmmad TahaОценок пока нет
- 2 Cholinergic BlockersДокумент49 страниц2 Cholinergic BlockersAmanuel MaruОценок пока нет
- MicrobiologyДокумент81 страницаMicrobiologyAmanuel MaruОценок пока нет
- 26 Biology 2 - 16 - 08 Cellular RespirationДокумент48 страниц26 Biology 2 - 16 - 08 Cellular RespirationAmanuel MaruОценок пока нет
- c03 PDFДокумент6 страницc03 PDFUloko ChristopherОценок пока нет
- 856 3443 1 PB PDFДокумент9 страниц856 3443 1 PB PDFAmanuel MaruОценок пока нет
- Health & Human BehaviorДокумент56 страницHealth & Human BehaviorAmanuel Maru100% (2)
- Intoduction To Clinical NursingДокумент58 страницIntoduction To Clinical NursingAmanuel MaruОценок пока нет
- Introduction To Medical Surgical NursingДокумент42 страницыIntroduction To Medical Surgical NursingAmanuel MaruОценок пока нет
- Chapter III Gram Positive RodsДокумент70 страницChapter III Gram Positive RodsAmanuel MaruОценок пока нет
- Pleural Disorders: 5/29/2018 1 by Shegaw Z (MSC in Ahn)Документ61 страницаPleural Disorders: 5/29/2018 1 by Shegaw Z (MSC in Ahn)Amanuel MaruОценок пока нет
- 1.household Water Supply and Basic SanitationДокумент8 страниц1.household Water Supply and Basic SanitationAmanuel MaruОценок пока нет
- Laboratory Diagnosis of Parasitic DiseasesДокумент57 страницLaboratory Diagnosis of Parasitic DiseasesAmanuel MaruОценок пока нет
- Basic concepts of computers explainedДокумент32 страницыBasic concepts of computers explainedabhi_txt90Оценок пока нет
- Ch.01 Introduction To ComputersДокумент10 страницCh.01 Introduction To ComputersSam Daka100% (1)
- Tayangan Organisasi Komputer D3 - TKДокумент358 страницTayangan Organisasi Komputer D3 - TKMelkie WalelignОценок пока нет
- Introduction To ComputingДокумент270 страницIntroduction To ComputingNadaОценок пока нет
- Biochemistry of Red Blood Cells (Erythrocytes) - : Rajesh.P. NarayananДокумент80 страницBiochemistry of Red Blood Cells (Erythrocytes) - : Rajesh.P. NarayananAmanuel MaruОценок пока нет
- PartyooДокумент1 страницаPartyooAmanuel MaruОценок пока нет
- General PathologyДокумент261 страницаGeneral PathologyHanif SharОценок пока нет
- 1,227 Qi FactsДокумент14 страниц1,227 Qi FactsMithilesh SinghОценок пока нет
- Computer-Basics - Computer Basics2Документ43 страницыComputer-Basics - Computer Basics2api-216226726Оценок пока нет
- Ajbms 2011 2 08Документ11 страницAjbms 2011 2 08Amanuel MaruОценок пока нет
- Bioch - of RBC CompleteДокумент88 страницBioch - of RBC CompleteAmanuel MaruОценок пока нет
- ICTFactsFigures2016 PDFДокумент8 страницICTFactsFigures2016 PDFPaulo HenriqueОценок пока нет
- Revision Resources s4-6Документ11 страницRevision Resources s4-6Amanuel MaruОценок пока нет
- Day 3Документ75 страницDay 3Amanuel MaruОценок пока нет
- GT PharmacodynamicsДокумент280 страницGT PharmacodynamicsAmanuel MaruОценок пока нет
- For PC-I Medicine Students By: Zelalem AДокумент39 страницFor PC-I Medicine Students By: Zelalem AAmanuel MaruОценок пока нет
- Unit 1Документ66 страницUnit 1Amanuel MaruОценок пока нет
- LeukemiaДокумент42 страницыLeukemiaAmanuel MaruОценок пока нет
- Assalamu'alaikum WR WB.: Emcee Script (1) Pre - AnnouncementДокумент3 страницыAssalamu'alaikum WR WB.: Emcee Script (1) Pre - AnnouncementGian AlfaОценок пока нет
- Signal WordsДокумент2 страницыSignal WordsJaol1976Оценок пока нет
- ProbabilityДокумент2 страницыProbabilityMickey WongОценок пока нет
- Subarachnoid Cisterns & Cerebrospinal FluidДокумент41 страницаSubarachnoid Cisterns & Cerebrospinal Fluidharjoth395Оценок пока нет
- BS 476-7-1997Документ24 страницыBS 476-7-1997Ivan ChanОценок пока нет
- Novel anti-tuberculosis strategies and nanotechnology-based therapies exploredДокумент16 страницNovel anti-tuberculosis strategies and nanotechnology-based therapies exploredArshia NazirОценок пока нет
- The Discrimination ModelДокумент16 страницThe Discrimination ModelSiti MuslihaОценок пока нет
- Importance of SimilesДокумент10 страницImportance of Similesnabeelajaved0% (1)
- Net Ionic EquationsДокумент8 страницNet Ionic EquationsCarl Agape DavisОценок пока нет
- WMCS Algebraic Simplification Grade 8 v1.0Документ76 страницWMCS Algebraic Simplification Grade 8 v1.0Vincent MartinОценок пока нет
- Ujpited ?tate of Americal: PresidentsДокумент53 страницыUjpited ?tate of Americal: PresidentsTino Acebal100% (1)
- New Intelligent AVR Controller Based On Particle Swarm Optimization For Transient Stability EnhancementДокумент6 страницNew Intelligent AVR Controller Based On Particle Swarm Optimization For Transient Stability EnhancementnaghamОценок пока нет
- Sta. Ignacia High School: Philosophy 101Документ1 страницаSta. Ignacia High School: Philosophy 101Mira VeranoОценок пока нет
- Experiment 5 ADHAVANДокумент29 страницExperiment 5 ADHAVANManoj Raj RajОценок пока нет
- Edukasyon Sa Pagpapakatao (Esp) Monitoring and Evaluation Tool For Department Heads/Chairmen/CoordinatorsДокумент3 страницыEdukasyon Sa Pagpapakatao (Esp) Monitoring and Evaluation Tool For Department Heads/Chairmen/CoordinatorsPrincis CianoОценок пока нет
- HexaflexДокумент10 страницHexaflexCharlie Williams100% (1)
- Yuri LotmanДокумент3 страницыYuri LotmanNHОценок пока нет
- Sovereignty of AllahДокумент1 страницаSovereignty of AllahmajjjidОценок пока нет
- Critters Table MannersДокумент3 страницыCritters Table Mannersapi-248006371Оценок пока нет
- Reducing Work Related Psychological Ill Health and Sickness AbsenceДокумент15 страницReducing Work Related Psychological Ill Health and Sickness AbsenceBM2062119PDPP Pang Kuok WeiОценок пока нет
- James A. Mcnamara JR.: An Interview WithДокумент22 страницыJames A. Mcnamara JR.: An Interview WithMiguel candelaОценок пока нет
- QHSE MANAGEMENT SYSTEM DOCUMENTATIONДокумент25 страницQHSE MANAGEMENT SYSTEM DOCUMENTATIONherisb100% (1)
- M5-2 CE 2131 Closed Traverse - Interior Angles V2021Документ19 страницM5-2 CE 2131 Closed Traverse - Interior Angles V2021Kiziahlyn Fiona BibayОценок пока нет
- Letter of Recommendation SamplesДокумент3 страницыLetter of Recommendation SamplesLahori MundaОценок пока нет
- Binomial TheoremДокумент57 страницBinomial Theoremkailasbankar96Оценок пока нет
- Second Periodic Test - 2018-2019Документ21 страницаSecond Periodic Test - 2018-2019JUVELYN BELLITAОценок пока нет
- Linux OS MyanmarДокумент75 страницLinux OS Myanmarweenyin100% (15)
- mc1776 - Datasheet PDFДокумент12 страницmc1776 - Datasheet PDFLg GnilОценок пока нет