Вам также может понравиться
- Antipsychotic Agents: CNS DrugsДокумент44 страницыAntipsychotic Agents: CNS DrugsJo Hn VengzОценок пока нет
- Cerebrovascular Accident PathophysiologyДокумент1 страницаCerebrovascular Accident PathophysiologyBerde KangleonОценок пока нет
- Depressive DisordersДокумент7 страницDepressive DisordersEllen JulianОценок пока нет
- Psychotropic Drugs: By: Rheajane Aguilar-RosalesДокумент77 страницPsychotropic Drugs: By: Rheajane Aguilar-Rosalesjean samson100% (1)
- Cephalgia PrimerДокумент2 страницыCephalgia PrimerVictor ChОценок пока нет
- Cefaleas 2018Документ87 страницCefaleas 2018Anonimo DesconocidoОценок пока нет
- Headache: An Overview: Danish Ejaz BhattiДокумент43 страницыHeadache: An Overview: Danish Ejaz BhattiPGHCОценок пока нет
- AntipsychoticsДокумент36 страницAntipsychoticsGlory MimiОценок пока нет
- Headache 2Документ11 страницHeadache 2khaled alahmadОценок пока нет
- 4 Headache Undergrad 2020Документ21 страница4 Headache Undergrad 2020b24trrznnrОценок пока нет
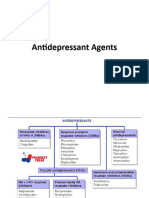
- Antidepressant AgentsДокумент45 страницAntidepressant Agentsmadeha goharОценок пока нет
- Journal Reading Syaraf-SuleДокумент45 страницJournal Reading Syaraf-SuleDrosophila Meilani GasterОценок пока нет
- Diskusi Topik (Sakit Kepala) - Nafisa Zulpa Elhapidi-406202067Документ34 страницыDiskusi Topik (Sakit Kepala) - Nafisa Zulpa Elhapidi-406202067nafisa zulfaelОценок пока нет
- Migraine and You: An Educational Guide For Migraine Headache SufferersДокумент23 страницыMigraine and You: An Educational Guide For Migraine Headache SufferersagelsantosОценок пока нет
- Antidepressants (ME216) 20 5Документ40 страницAntidepressants (ME216) 20 5Dineish MurugaiahОценок пока нет
- SESSION 09 PharmacotherapyДокумент69 страницSESSION 09 PharmacotherapyMalakatete Mwaipojele-fОценок пока нет
- Unit 2 Anti Migraine and Drugs For Trigeminal Neuralgia Pharmacy-IIДокумент38 страницUnit 2 Anti Migraine and Drugs For Trigeminal Neuralgia Pharmacy-IIAsad MirajОценок пока нет
- Palliative and End of Life CareДокумент19 страницPalliative and End of Life CarePranjal KothaleОценок пока нет
- 2 MigraineДокумент3 страницы2 MigraineTommy ArisandyОценок пока нет
- Antidepressants (Igor Iezhitsa) Students Copy (ME219)Документ40 страницAntidepressants (Igor Iezhitsa) Students Copy (ME219)Zobayer AhmedОценок пока нет
- Tramadol and Akisol: by Wael Hamdan, Samah Makki, Ahmed Zahir, SallyДокумент23 страницыTramadol and Akisol: by Wael Hamdan, Samah Makki, Ahmed Zahir, SallyMohamedОценок пока нет
- Headache: Migraine and Tension-Type HeadacheДокумент12 страницHeadache: Migraine and Tension-Type HeadacheLoren SangalangОценок пока нет
- Tension Type HeadacheДокумент18 страницTension Type HeadacheRiris SihotangОценок пока нет
- Management of Bipolar DisordersДокумент18 страницManagement of Bipolar Disorderss67346446Оценок пока нет
- Fibromyalgia: An Update On Clinical Characteristics, Aetiopathogenesis and TreatmentДокумент25 страницFibromyalgia: An Update On Clinical Characteristics, Aetiopathogenesis and TreatmenthansenОценок пока нет
- Management of Migraine Headaches in A Chronic Pain Patient: A Case ReportДокумент5 страницManagement of Migraine Headaches in A Chronic Pain Patient: A Case Reporthenandwitafadilla28Оценок пока нет
- Headache: & Associated EmergenciesДокумент63 страницыHeadache: & Associated EmergenciesMahad IbrahemОценок пока нет
- Stephen Silberstein - Medication Overuse HeadacheДокумент2 страницыStephen Silberstein - Medication Overuse HeadacheAnHy HandayaniОценок пока нет
- Headache Disorder and Pain ManagementДокумент11 страницHeadache Disorder and Pain ManagementDaenica Lorraine Abella SebastianОценок пока нет
- Primary Headache: Mohamad Dawoud 6 Course Kharkiv National Medical UniversityДокумент17 страницPrimary Headache: Mohamad Dawoud 6 Course Kharkiv National Medical UniversityMhamad DawoudОценок пока нет
- Bipolar Lecture11Документ5 страницBipolar Lecture11hhanono924097Оценок пока нет
- Treatments in PsychiatryДокумент31 страницаTreatments in PsychiatryChro MAОценок пока нет
- Antidepressants Ssris, Snris: Selective Serotonin Reuptake Inhibitors Norepinephrine Reuptake InhibitorsДокумент23 страницыAntidepressants Ssris, Snris: Selective Serotonin Reuptake Inhibitors Norepinephrine Reuptake InhibitorsJosh SchultzОценок пока нет
- PSYCHOPHARMACOLOGYДокумент35 страницPSYCHOPHARMACOLOGYsalehaqamer64Оценок пока нет
- PsychopharmacologyДокумент32 страницыPsychopharmacologyCms CSU100% (1)
- Analgesic & Anesthetic: Dr. Yunita Sari Pane, MsiДокумент92 страницыAnalgesic & Anesthetic: Dr. Yunita Sari Pane, Msiqori fadillahОценок пока нет
- Drugs Acting On The Nervous SystemДокумент123 страницыDrugs Acting On The Nervous SystemIretiola Adeleru100% (1)
- Drugs Acting On The Nervous SystemДокумент123 страницыDrugs Acting On The Nervous SystemIretiola AdeleruОценок пока нет
- Psych DrugsДокумент46 страницPsych DrugsDaniela OrtalОценок пока нет
- Chapter 2 Neurobiologic Theories and Psycho PharmacologyДокумент36 страницChapter 2 Neurobiologic Theories and Psycho PharmacologyPrecious Pearl Tadena100% (1)
- WEEK 6 PPT PainДокумент22 страницыWEEK 6 PPT PainDanica FrancoОценок пока нет
- 4 HeadacheДокумент33 страницы4 HeadacheNathaniel BudayОценок пока нет
- Anti-Anxiety ag-WPS OfficeДокумент8 страницAnti-Anxiety ag-WPS Officermconvidhya sri2015Оценок пока нет
- Psychopharmacology - Dr. Citra Ayu Aprilia, M.kes - Rabu 19 Oktober 2022 - 07.00 - 08.50 - EditДокумент99 страницPsychopharmacology - Dr. Citra Ayu Aprilia, M.kes - Rabu 19 Oktober 2022 - 07.00 - 08.50 - EditCITRA AYU APRILIAОценок пока нет
- HeadacheДокумент36 страницHeadacheabenezer g/kirstosОценок пока нет
- 1PainAssessment - Pharmokinetics - 2018 Jeannies EditДокумент54 страницы1PainAssessment - Pharmokinetics - 2018 Jeannies EditApostolos T.Оценок пока нет
- Graves Disease Treated With Classical Homeopathy: by Thomas R. Firor, M.DДокумент2 страницыGraves Disease Treated With Classical Homeopathy: by Thomas R. Firor, M.DSiva PathasekaranОценок пока нет
- Psychiatry Shelf ReviewДокумент11 страницPsychiatry Shelf ReviewAhmad Syahmi YZ75% (4)
- Pharmacology of Mood Stabilizers: DR - Datten Bangun, MSC, SPFK Dept - Farmakologi & Terapetik Fak - Kedokteran Uhn MedanДокумент51 страницаPharmacology of Mood Stabilizers: DR - Datten Bangun, MSC, SPFK Dept - Farmakologi & Terapetik Fak - Kedokteran Uhn MedanFansisca SiallaganОценок пока нет
- Management of Major Depressive DisorderДокумент14 страницManagement of Major Depressive DisorderKwongjong LiОценок пока нет
- Antidepressant DrugsДокумент15 страницAntidepressant DrugsDr. Mushfique Imtiaz ChowdhuryОценок пока нет
- Neuro - 1 - Template - HeadacheДокумент43 страницыNeuro - 1 - Template - Headacheabhi wagleОценок пока нет
- AntidepressantsДокумент4 страницыAntidepressantsSalman HabeebОценок пока нет
- Psychopharmacological AgentsДокумент44 страницыPsychopharmacological Agentsbazet49Оценок пока нет
- Module-10-Lecture-4 - Cannabis, Mental Health, and Brain DisordersДокумент13 страницModule-10-Lecture-4 - Cannabis, Mental Health, and Brain DisordersAbdul Aziz Success CoachОценок пока нет
- Treatment of Schizophrenia and Management of Drug SideДокумент83 страницыTreatment of Schizophrenia and Management of Drug SideAbelОценок пока нет
- Migraine Headache: in Partial Fulfillment of Nursing 505B by Melissa A. MakhoulДокумент26 страницMigraine Headache: in Partial Fulfillment of Nursing 505B by Melissa A. MakhoulMelissa MakhoulОценок пока нет
- Generalized Anxiety DisorderДокумент3 страницыGeneralized Anxiety DisorderAhmad Syahmi YZОценок пока нет
- Migraines: Migraine Treatment and Prevention Options: The most important information you need to improve your healthОт EverandMigraines: Migraine Treatment and Prevention Options: The most important information you need to improve your healthОценок пока нет
- Depression & Anxiety: What You Need To Know About Treatment with Medications, Herbs & SupplementsОт EverandDepression & Anxiety: What You Need To Know About Treatment with Medications, Herbs & SupplementsОценок пока нет
- Medical Encyclopedia XXL: Prof. J.P. Schadé, M.D., Ph.D. D.Sc.hcОт EverandMedical Encyclopedia XXL: Prof. J.P. Schadé, M.D., Ph.D. D.Sc.hcОценок пока нет
- Fragile XДокумент10 страницFragile Xryan20eОценок пока нет
- HyperglycemiaДокумент3 страницыHyperglycemiadaks89Оценок пока нет
- Traumatic Brain Injury Cause Non-Traumatic Brain Injury CausesДокумент10 страницTraumatic Brain Injury Cause Non-Traumatic Brain Injury CausesBaoz PingОценок пока нет
- Stroke: Nivedita MPT (Neuro)Документ27 страницStroke: Nivedita MPT (Neuro)MenakaОценок пока нет
- Genogram Diagram - Part 1Документ1 страницаGenogram Diagram - Part 1api-609737816Оценок пока нет
- Psychosomatic DisordersДокумент11 страницPsychosomatic DisordersJasmin Jacob100% (3)
- Ocd EssayДокумент3 страницыOcd EssayTheGreatHelperОценок пока нет
- 3b.DELUSINAL DISORDERSДокумент14 страниц3b.DELUSINAL DISORDERSIano IanoОценок пока нет
- Isaac Sydrome Case ReportДокумент6 страницIsaac Sydrome Case Reportishan130890Оценок пока нет
- ZidukixobeДокумент3 страницыZidukixobeرمزي سويسيОценок пока нет
- CMQCC - Maternal Early Warning SystemДокумент3 страницыCMQCC - Maternal Early Warning SystemDesi WildayaniОценок пока нет
- Assessment NCM 101Документ1 страницаAssessment NCM 101Lorainne Angel U. MolinaОценок пока нет
- Michael B First Et Al - SCID 5-RV Structured Clinical Interview For DSM 5 Diagnoses Research Version - Libgen - LiДокумент223 страницыMichael B First Et Al - SCID 5-RV Structured Clinical Interview For DSM 5 Diagnoses Research Version - Libgen - LiosiixyОценок пока нет
- Jipmat 2023Документ46 страницJipmat 2023Aditya Nath ChaudharyОценок пока нет
- The Mental Status Examination: Dr. Ramesh Parmar Department of Psychiatry PDU Medical College, RajkotДокумент33 страницыThe Mental Status Examination: Dr. Ramesh Parmar Department of Psychiatry PDU Medical College, RajkotRamashanker YadavОценок пока нет
- WSR II - July 11 2022Документ5 страницWSR II - July 11 2022ال حلفاويОценок пока нет
- CPR Quiz - Kahoot!Документ10 страницCPR Quiz - Kahoot!jayshondedrick7Оценок пока нет
- SOCA 2008 - Semester 6Документ1 страницаSOCA 2008 - Semester 6Devina HarsonoОценок пока нет
- Resume PsychologyДокумент5 страницResume PsychologyMuhammad SlametОценок пока нет
- Clinical Psych BookletДокумент36 страницClinical Psych BookletNancy MohamedОценок пока нет
- Running Head: CASE STUDY 1 1Документ9 страницRunning Head: CASE STUDY 1 1ElizaIancuОценок пока нет
- Quantum Reflex IntegrationДокумент2 страницыQuantum Reflex IntegrationAarif SharifОценок пока нет
- DRSABCDДокумент4 страницыDRSABCDBilalОценок пока нет
- Initial Assesment: Penilaian Awalpasien Gawat DaruratДокумент32 страницыInitial Assesment: Penilaian Awalpasien Gawat DaruratYusrilОценок пока нет
- What Is Coprolalia, Tourette's SyndromeДокумент3 страницыWhat Is Coprolalia, Tourette's Syndromehttp://feelgoodtime.netОценок пока нет
- The New Clasification ILAE 2017Документ6 страницThe New Clasification ILAE 2017Ami D ALОценок пока нет
- Internal Disc Disruption ArticleДокумент2 страницыInternal Disc Disruption ArticleHazem BОценок пока нет
- Chapter 2Документ2 страницыChapter 2Castro RicОценок пока нет
- Screen For Child Anxiety Related DisordersДокумент4 страницыScreen For Child Anxiety Related DisordersFebri Tri HamunanganОценок пока нет