Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
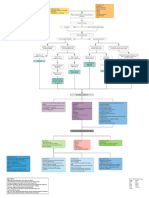
- Myocardial Infarction With CABG Concept MapДокумент1 страницаMyocardial Infarction With CABG Concept MapMaria Therese100% (1)
- PACU Monitoring Sheet - RR Record - SCT-CONДокумент4 страницыPACU Monitoring Sheet - RR Record - SCT-CONFitz JaminitОценок пока нет
- NMND 5103 Assignment 2Документ49 страницNMND 5103 Assignment 2Sithara JayatungaОценок пока нет
- Post Stroke Scalp AcupunctureДокумент64 страницыPost Stroke Scalp AcupunctureJosé Mário91% (11)
- Characteristics & Diagnosis: What Is Autism?Документ2 страницыCharacteristics & Diagnosis: What Is Autism?Fire LadОценок пока нет
- Chemicals, Pharmaceuticals, Oil, Dairy, Food, Beverages, Paint & Others Industry DetailsДокумент12 страницChemicals, Pharmaceuticals, Oil, Dairy, Food, Beverages, Paint & Others Industry DetailsSuzikline Engineering100% (1)
- Kinesio Taping: Done By: Rawan Al DhabiДокумент29 страницKinesio Taping: Done By: Rawan Al DhabiJovelle DasallaОценок пока нет
- Skin Rashes in ChildrenДокумент11 страницSkin Rashes in ChildrenwiladamanikОценок пока нет
- Acromegaly and GigantismДокумент4 страницыAcromegaly and GigantismnfacmaОценок пока нет
- Trends in Nursing Practice-2Документ36 страницTrends in Nursing Practice-2nithya nithyaОценок пока нет
- Indian AdministrationДокумент52 страницыIndian Administrationcitidotnet100% (1)
- Contagious Diseases in PHДокумент10 страницContagious Diseases in PHJEnLipataОценок пока нет
- Internal HemmorhoidsДокумент5 страницInternal Hemmorhoids2netvelasquezОценок пока нет
- IARC Monograph - Carcinogen PDFДокумент498 страницIARC Monograph - Carcinogen PDFEma KusumaОценок пока нет
- Public Health CareДокумент11 страницPublic Health CareFemale calmОценок пока нет
- Principles of Aseptic TechniqueДокумент5 страницPrinciples of Aseptic TechniqueNicole Audrey JoaquinОценок пока нет
- PHARMACY AND THERAPEUTICS COMMITTEE Edited 12345Документ38 страницPHARMACY AND THERAPEUTICS COMMITTEE Edited 12345Shafaqat Ghani Shafaqat Ghani100% (3)
- Documentation of Medical Evidence For Disability Evaluation PurposesДокумент5 страницDocumentation of Medical Evidence For Disability Evaluation PurposesJim100% (2)
- Ophthalmia NeonatorumДокумент17 страницOphthalmia NeonatorumIndranil DuttaОценок пока нет
- PR Design Rpoblem 200 Bed G. HospitalДокумент6 страницPR Design Rpoblem 200 Bed G. HospitalFreiya - Jane UndayОценок пока нет
- Clinical LeadersДокумент2 страницыClinical LeadersInfoJDJОценок пока нет
- BREASTFEEDINGДокумент2 страницыBREASTFEEDINGFianisa RizkaОценок пока нет
- 11.3 MGR UniversityДокумент15 страниц11.3 MGR UniversityValarmathiОценок пока нет
- Palmer - Final CoachingДокумент9 страницPalmer - Final CoachingDonald SebidanОценок пока нет
- 4564 2934 p436 Pages Deleted EditedДокумент4 страницы4564 2934 p436 Pages Deleted EditedHaniОценок пока нет
- Cardiology BrochureДокумент2 страницыCardiology Brochureong251183Оценок пока нет
- 5 Storyboard (Contoh 1)Документ1 страница5 Storyboard (Contoh 1)RaniCianTarОценок пока нет
- Ahmad Abid Bin Abas 07-5-2 Ahmad Asyraf Bin Mohamed 07-5-3Документ8 страницAhmad Abid Bin Abas 07-5-2 Ahmad Asyraf Bin Mohamed 07-5-3sandeepОценок пока нет
- Alginate ImpressionДокумент60 страницAlginate ImpressionNugraha AnggaОценок пока нет
- Weekly Home Learning Plan in Pe and Health 12 Date: - Teacher: Rojelyn Santiago Submitted TP: Dr. Rebecca F. AverionДокумент2 страницыWeekly Home Learning Plan in Pe and Health 12 Date: - Teacher: Rojelyn Santiago Submitted TP: Dr. Rebecca F. AverionpdhgfgbdОценок пока нет