Вам также может понравиться
- Gynecology: Three Minimally Invasive Procedures You Need to Know About For: Permanent Birth Control, Heavy Menstrual Periods, Accidental Loss of Urine Plus: Modern Hormone Therapy for the Post Menopausal WomenОт EverandGynecology: Three Minimally Invasive Procedures You Need to Know About For: Permanent Birth Control, Heavy Menstrual Periods, Accidental Loss of Urine Plus: Modern Hormone Therapy for the Post Menopausal WomenОценок пока нет
- IUCDДокумент24 страницыIUCDcropsandinsects100% (1)
- IudsДокумент75 страницIudssunielgowdaОценок пока нет
- Intra Uterine Device: Ruswana Anwar, DR, Spog (K), MkesДокумент69 страницIntra Uterine Device: Ruswana Anwar, DR, Spog (K), MkesMochammad Rizal AttamimiОценок пока нет
- Intrauterine Drug Delivery SystemДокумент33 страницыIntrauterine Drug Delivery SystemAmit Belekar100% (1)
- DefinitionДокумент12 страницDefinitionalfiОценок пока нет
- Intra-Uterine Contraceptive Device (Iucd) Letchy FourieДокумент14 страницIntra-Uterine Contraceptive Device (Iucd) Letchy FourieNyakie MotlalaneОценок пока нет
- Intrauterine Contraceptive DevicesДокумент15 страницIntrauterine Contraceptive DevicesAditya Malladi100% (1)
- Intrauterine Device (IUD)Документ46 страницIntrauterine Device (IUD)semegn0936Оценок пока нет
- Family Planning Methods/ Contraceptive Methods/nurses Education/ B.Sc. NursingДокумент129 страницFamily Planning Methods/ Contraceptive Methods/nurses Education/ B.Sc. NursingSameekshaОценок пока нет
- Artificial Family Planning Methods Artificial Family Planning MethodsДокумент33 страницыArtificial Family Planning Methods Artificial Family Planning MethodsJullienne Ysabelle AngОценок пока нет
- Intrauterine Devices: By: Widi Cahya Utami MentorДокумент11 страницIntrauterine Devices: By: Widi Cahya Utami MentorAry JossОценок пока нет
- Group 4 Artificial MethodДокумент19 страницGroup 4 Artificial MethodDonah Marie Dumago AtanacioОценок пока нет
- Copper IUD: Wilson's Disease LNG-IUD: Progestin-DependentДокумент2 страницыCopper IUD: Wilson's Disease LNG-IUD: Progestin-DependentTyler VintОценок пока нет
- Long-Acting Reversible Contraceptive (LARC)Документ29 страницLong-Acting Reversible Contraceptive (LARC)temitope ogunfowokanОценок пока нет
- Update IUD Overview 2020 08Документ21 страницаUpdate IUD Overview 2020 08Laurențiu LucaОценок пока нет
- 08.04.20-AF, Unit-12, Family Wefare Programme, - Methods of contraception-8.04.20-ANДокумент65 страниц08.04.20-AF, Unit-12, Family Wefare Programme, - Methods of contraception-8.04.20-ANElakkiyaanu64 Elakkiyaanu64Оценок пока нет
- Copper T InsertionДокумент19 страницCopper T Insertionapi-3823785100% (2)
- AKDR Hormonal Dan Non HormonalДокумент35 страницAKDR Hormonal Dan Non Hormonalradhiah karimОценок пока нет
- Family PlanningДокумент98 страницFamily PlanningDonnaBells Hermo Labaniego50% (2)
- Family Planning MethodsДокумент71 страницаFamily Planning MethodsFranklin Thomas100% (1)
- Intrauterine Contraceptive Device (Iud)Документ37 страницIntrauterine Contraceptive Device (Iud)Madhavaraj SNОценок пока нет
- Contraception MethodsДокумент15 страницContraception Methodsyash myatraОценок пока нет
- PPIUDДокумент16 страницPPIUDmusicwizardОценок пока нет
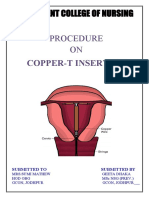
- Procedure ON: Copper-T InsertionДокумент5 страницProcedure ON: Copper-T Insertionpriyanka100% (2)
- DR Amirah Zainab Binti Mamat @muhammadДокумент45 страницDR Amirah Zainab Binti Mamat @muhammadAmirah MuhammadОценок пока нет
- Permanent Family PlanningДокумент36 страницPermanent Family PlanningNilakshi Barik MandalОценок пока нет
- Family Planning: CC Bernabe Excelsior 2017Документ51 страницаFamily Planning: CC Bernabe Excelsior 2017Jessa MaeОценок пока нет
- Group 3 - MOW (Medical Oprative Women) Tubectomy and IUDДокумент13 страницGroup 3 - MOW (Medical Oprative Women) Tubectomy and IUDIrfinaОценок пока нет
- The Intrauterine Device: HealthДокумент2 страницыThe Intrauterine Device: HealthApris Tesryanto LiufetoОценок пока нет
- EndometritisДокумент21 страницаEndometritisRoshni SunarОценок пока нет
- C12 P13 TubectomyДокумент24 страницыC12 P13 TubectomyRaviKurleОценок пока нет
- 2023.07.17 - Obstetrice S2. 03 - Family Planning ContraceptionДокумент88 страниц2023.07.17 - Obstetrice S2. 03 - Family Planning ContraceptionVignesh ThangavelОценок пока нет
- Long-Term Safety, Efficacy, and Patient Acceptabilty of The Intraurine Copper T-380A Contraceptive DeviceДокумент14 страницLong-Term Safety, Efficacy, and Patient Acceptabilty of The Intraurine Copper T-380A Contraceptive DeviceGary WirawanОценок пока нет
- Objective: Fig.1. Copper T 200 B With Insertion Tube, Flange and PlungerДокумент19 страницObjective: Fig.1. Copper T 200 B With Insertion Tube, Flange and Plungerahilesh_babuОценок пока нет
- Long-Term Safety, Efficacy, and Patient Acceptability of The Intrauterine Copper T-380A Contraceptive DeviceДокумент10 страницLong-Term Safety, Efficacy, and Patient Acceptability of The Intrauterine Copper T-380A Contraceptive DeviceelmaildejosejuanОценок пока нет
- Family Planning and ContraceptionДокумент39 страницFamily Planning and ContraceptionDitaleniОценок пока нет
- Lecture 18family PlanningДокумент44 страницыLecture 18family PlanningSulaiman SanusiОценок пока нет
- Circ LageДокумент54 страницыCirc Lagetsega tilahunОценок пока нет
- Tubal LigationДокумент14 страницTubal LigationGrace Ann DacuanОценок пока нет
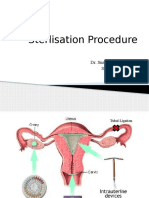
- Sterlisation Procedure: Dr. Sushruta Shrivastava SR Dept of OBGY AIIMS, BhopalДокумент30 страницSterlisation Procedure: Dr. Sushruta Shrivastava SR Dept of OBGY AIIMS, BhopalsushrutaОценок пока нет
- Mechanisms of ActionДокумент3 страницыMechanisms of ActionMitch C.Оценок пока нет
- Cervical Incompetence: DR - Asmita Pantha Resident, OBGYNДокумент36 страницCervical Incompetence: DR - Asmita Pantha Resident, OBGYNshrinkhala bhattaraiОценок пока нет
- 46s - Contraception TBL (Pearson - Dillon)Документ13 страниц46s - Contraception TBL (Pearson - Dillon)adriaran101Оценок пока нет
- Family PlanningДокумент16 страницFamily PlanningMy StoryОценок пока нет
- Family PlanningДокумент20 страницFamily PlanningAyush PaudelОценок пока нет
- Fertility Control: Shah Fahad Demonstrator Rehman College of Allied Health SciencesДокумент11 страницFertility Control: Shah Fahad Demonstrator Rehman College of Allied Health SciencesSalman KhanОценок пока нет
- Insertion and Removal of Intrauterine Devices-AAFPДокумент8 страницInsertion and Removal of Intrauterine Devices-AAFPnouval_iqbalОценок пока нет
- Peace Corps MTG 700 General Medicine 2Документ191 страницаPeace Corps MTG 700 General Medicine 2Accessible Journal Media: Peace Corps DocumentsОценок пока нет
- 9 IucdДокумент10 страниц9 IucdHaileyesus NatnaelОценок пока нет
- Family Planning HabtamuДокумент106 страницFamily Planning HabtamukakujirexОценок пока нет
- Contraception - Updates: Mr. Wu Pin Ms. Nur SakinahДокумент66 страницContraception - Updates: Mr. Wu Pin Ms. Nur SakinahHanif GandohОценок пока нет
- Family Planning - 4Документ8 страницFamily Planning - 4Khibul LimОценок пока нет
- Intra Uterine Device: (Iud) / AkdrДокумент16 страницIntra Uterine Device: (Iud) / AkdrelsahewuniОценок пока нет
- How Can A Small Piece of Copper Prevent You From Getting Pregnant?Документ4 страницыHow Can A Small Piece of Copper Prevent You From Getting Pregnant?Dharmendra SinghОценок пока нет
- WK 16 Cerv Can ValerianoДокумент2 страницыWK 16 Cerv Can ValerianoVALERIANO TRISHAОценок пока нет
- Family Planning Methods: Presented byДокумент56 страницFamily Planning Methods: Presented byNise Mon KuriakoseОценок пока нет
- Research - Long Version 2Документ87 страницResearch - Long Version 2Erika LlorenОценок пока нет
- CT CervicalДокумент2 страницыCT CervicalPrincess Laira CañeteОценок пока нет
- Journal TyphoidДокумент4 страницыJournal TyphoidImaylani S. SitanggangОценок пока нет
- LapjagДокумент5 страницLapjagImaylani S. SitanggangОценок пока нет
- Nephrology Lupus UpdateДокумент11 страницNephrology Lupus UpdateLoredana GhercăОценок пока нет
- Diagnostic Value of Widal Test in The Diagnosis of Typhoid Fever Asystematic Review 2161 0703 1000248Документ4 страницыDiagnostic Value of Widal Test in The Diagnosis of Typhoid Fever Asystematic Review 2161 0703 1000248eko andryОценок пока нет
- Jurnal Radiologi ClaraДокумент9 страницJurnal Radiologi ClaraImaylani S. SitanggangОценок пока нет
- How To Write A Case Study PDFДокумент4 страницыHow To Write A Case Study PDFMatthew Osei-NkrumahОценок пока нет
- Management of Severe Acute Malnutrition: Jeané CloeteДокумент15 страницManagement of Severe Acute Malnutrition: Jeané CloeteImaylani S. SitanggangОценок пока нет
- Cover Jurding DR AdeДокумент1 страницаCover Jurding DR AdeImaylani S. SitanggangОценок пока нет
- Carpal Tunnel Syndrome JurnalДокумент9 страницCarpal Tunnel Syndrome JurnalImaylani S. SitanggangОценок пока нет
- Veterinarian Surgery in Operation Room PowerPoint Templates StandardДокумент2 страницыVeterinarian Surgery in Operation Room PowerPoint Templates StandardImaylani S. SitanggangОценок пока нет
- Journal Gyn KETДокумент8 страницJournal Gyn KETImaylani S. SitanggangОценок пока нет
- List Barang Animal LabДокумент2 страницыList Barang Animal LabImaylani S. SitanggangОценок пока нет
- Pulmo DLLДокумент5 страницPulmo DLLImaylani S. SitanggangОценок пока нет
- Adore You - PDFДокумент290 страницAdore You - PDFnbac0dОценок пока нет
- Queen - Hammer To Fall ChordsДокумент3 страницыQueen - Hammer To Fall ChordsDavideContiОценок пока нет
- Biology Concepts and Applications 9th Edition Starr Solutions ManualДокумент9 страницBiology Concepts and Applications 9th Edition Starr Solutions Manualscarletwilliamnfz100% (31)
- 2062 TSSR Site Sharing - Rev02Документ44 страницы2062 TSSR Site Sharing - Rev02Rio DefragОценок пока нет
- FoodhallДокумент3 страницыFoodhallswopnilrohatgiОценок пока нет
- Goodman Aula 1 e 2Документ17 страницGoodman Aula 1 e 2Danilo TetОценок пока нет
- Standards Guide 1021 1407Документ8 страницStandards Guide 1021 1407Anjur SiОценок пока нет
- Copy - of - Commonlit - Meet The Fearless Cook Who Secretly Fed and Funded The Civil Rights Movement - StudentДокумент6 страницCopy - of - Commonlit - Meet The Fearless Cook Who Secretly Fed and Funded The Civil Rights Movement - Studentlilywright08Оценок пока нет
- Luigi Cherubini Requiem in C MinorДокумент8 страницLuigi Cherubini Requiem in C MinorBen RutjesОценок пока нет
- Software Requirements SpecificationДокумент9 страницSoftware Requirements SpecificationSu-kEm Tech LabОценок пока нет
- 15-3-2020 Chapter 4 Forward Kinematics Lecture 1Документ29 страниц15-3-2020 Chapter 4 Forward Kinematics Lecture 1MoathОценок пока нет
- Pinto pm5 Tif 02Документ24 страницыPinto pm5 Tif 02Salem BawazirОценок пока нет
- The Accreditation Committee Cityland Development CorporationДокумент5 страницThe Accreditation Committee Cityland Development Corporationthe apprenticeОценок пока нет
- Genstat Release 10.3de (Pc/Windows 7) 28 May 2012 06:35:59Документ6 страницGenstat Release 10.3de (Pc/Windows 7) 28 May 2012 06:35:59Anna Nur HidayatiОценок пока нет
- CP AssignmentДокумент5 страницCP AssignmentMSSM EngineeringОценок пока нет
- E34-1 Battery Charging and Dishcharging BoardДокумент23 страницыE34-1 Battery Charging and Dishcharging BoardGanesa MurthyОценок пока нет
- Upend RA Kumar: Master List of Approved Vendors For Manufacture and Supply of Electrical ItemsДокумент42 страницыUpend RA Kumar: Master List of Approved Vendors For Manufacture and Supply of Electrical Itemssantosh iyerОценок пока нет
- Business Maths Chapter 5Документ9 страницBusiness Maths Chapter 5鄭仲抗Оценок пока нет
- Asin URL Index URL/keyword DomainДокумент30 страницAsin URL Index URL/keyword DomainStart AmazonОценок пока нет
- Making Sense of The Future of Libraries: Dan Dorner, Jennifer Campbell-Meier and Iva SetoДокумент14 страницMaking Sense of The Future of Libraries: Dan Dorner, Jennifer Campbell-Meier and Iva SetoBiblioteca IICEОценок пока нет
- DS WhitePaper Troubleshooting 3DEXPERIENCE ABEND SituationsДокумент26 страницDS WhitePaper Troubleshooting 3DEXPERIENCE ABEND SituationsSam AntonyОценок пока нет
- Study of Bond Properties of Concrete Utilizing Fly Ash, Marble and Granite PowderДокумент3 страницыStudy of Bond Properties of Concrete Utilizing Fly Ash, Marble and Granite PowderLegaldevil LlabsОценок пока нет
- PCI Secure Software Standard v1 - 0Документ67 страницPCI Secure Software Standard v1 - 0Antonio ClimaОценок пока нет
- Grade 10 LP Thin LensДокумент6 страницGrade 10 LP Thin LensBrena PearlОценок пока нет
- Ojt HRMДокумент7 страницOjt HRMArlyn Joy NacinoОценок пока нет
- Omegas Prezentacija 01Документ20 страницOmegas Prezentacija 01Predrag Djordjevic100% (1)
- Esp 1904 A - 70 TPH o & M ManualДокумент50 страницEsp 1904 A - 70 TPH o & M Manualpulakjaiswal85Оценок пока нет
- Glossario - GETTY - IngДокумент24 страницыGlossario - GETTY - IngFabio ZarattiniОценок пока нет
- Trading Book - AGДокумент7 страницTrading Book - AGAnilkumarGopinathanNairОценок пока нет