Вам также может понравиться
- Clinical Utility of Multiphasic Questionnaire MPQ - 39 42Документ5 страницClinical Utility of Multiphasic Questionnaire MPQ - 39 42DN100% (1)
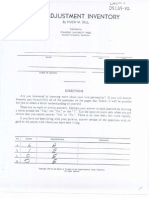
- Bell Adjustment Inventory (1934)Документ4 страницыBell Adjustment Inventory (1934)sherrybrar100% (3)
- Yale Brown Obsessive Compulsive ScaleДокумент2 страницыYale Brown Obsessive Compulsive ScaleUm Ar100% (1)
- Unit 1 Clinical PsychologyДокумент26 страницUnit 1 Clinical PsychologyRoshan100% (1)
- House Tree Person Interpretation ElementsДокумент6 страницHouse Tree Person Interpretation Elementsnesuma75% (8)
- House Tree Person Interpretation ElementsДокумент6 страницHouse Tree Person Interpretation Elementsnesuma75% (8)
- Wonderland Audition PacketДокумент5 страницWonderland Audition PacketBritt Boyd100% (1)
- Behavioural Sciences Unit 1 - Introduction: Pure PsychologyДокумент19 страницBehavioural Sciences Unit 1 - Introduction: Pure PsychologybettykoshyОценок пока нет
- Psychological Test Price List 2009Документ54 страницыPsychological Test Price List 2009Meenu Minu67% (9)
- Projective TechniquesДокумент38 страницProjective TechniquesMs. Rachel SamsonОценок пока нет
- An Etymological Dictionary of The Scottivol 2Документ737 страницAn Etymological Dictionary of The Scottivol 2vstrohmeОценок пока нет
- M Phil Clinical PsychologyДокумент41 страницаM Phil Clinical PsychologyNazema_SagiОценок пока нет
- 37 Sample Resolutions Very Useful, Indian Companies Act, 1956Документ38 страниц37 Sample Resolutions Very Useful, Indian Companies Act, 1956CA Vaibhav Maheshwari70% (23)
- Psychological Testing-II Report Submitted by Fatima Syed Fa17-Bpy-016Документ53 страницыPsychological Testing-II Report Submitted by Fatima Syed Fa17-Bpy-016Fatima SyedОценок пока нет
- Operant ConditioningДокумент76 страницOperant ConditioningJiya JanjuaОценок пока нет
- Clinical PsychologyДокумент54 страницыClinical PsychologyJana ChihaiОценок пока нет
- Unit 4 - Behavior TherapyДокумент32 страницыUnit 4 - Behavior TherapyKashish Bajaj100% (1)
- Psychological Disorders: AP Psychology Mr. HollandДокумент20 страницPsychological Disorders: AP Psychology Mr. Hollandyummywords1254Оценок пока нет
- Psychology ReviewerДокумент7 страницPsychology ReviewerGrazielle Anne SancejaОценок пока нет
- ISAA ToolДокумент21 страницаISAA Toolkrishnaveni arulkumarОценок пока нет
- Observational Study: Supervised by - DR SAKSHI MEHROTRA Submitted by - Ananya BhattacharjeeДокумент11 страницObservational Study: Supervised by - DR SAKSHI MEHROTRA Submitted by - Ananya BhattacharjeeManik DagarОценок пока нет
- Psychological TestingДокумент12 страницPsychological TestingUniversity of Madras International Conference100% (2)
- ABC Checklist Duration Intensity DataGC1Документ1 страницаABC Checklist Duration Intensity DataGC1Um ArОценок пока нет
- Maudsleys Personality InventoryДокумент4 страницыMaudsleys Personality InventorySatya Rajesh IyerОценок пока нет
- Industrial PsychologyДокумент38 страницIndustrial Psychologysheetalkaurahuja57% (7)
- Answers To Quiz No 19Документ5 страницAnswers To Quiz No 19Your Public Profile100% (4)
- Health Belief ModelДокумент2 страницыHealth Belief ModelEllen Michelle MaestradoОценок пока нет
- Moving Quiz - Chapter 1 and 2 Positive PsychologyДокумент28 страницMoving Quiz - Chapter 1 and 2 Positive PsychologyRhalf100% (1)
- Lect 2 What Is Clinical Psychology PostingДокумент31 страницаLect 2 What Is Clinical Psychology PostingumibrahimОценок пока нет
- Behaviour Therapy NotesДокумент5 страницBehaviour Therapy NotesDipti Punjal100% (1)
- Developmental Psychology Lecture NotesДокумент44 страницыDevelopmental Psychology Lecture NotesEva BeunkОценок пока нет
- Rotter Incomplete Sentence BlankДокумент8 страницRotter Incomplete Sentence BlankIshtiaq AhmadОценок пока нет
- Humanistic Approach To CounsellingДокумент2 страницыHumanistic Approach To CounsellingJoseph Hong100% (2)
- Industrial PsychologyДокумент227 страницIndustrial PsychologyAya Aishi100% (1)
- Conditions Influencing CounsellingДокумент4 страницыConditions Influencing Counsellingsinghsanya100% (1)
- Mental Health Inventory - 220808 - 100604Документ14 страницMental Health Inventory - 220808 - 100604Sunil Rathod100% (2)
- PEG Catalog Siemens PDFДокумент419 страницPEG Catalog Siemens PDFrukmagoudОценок пока нет
- Health Psychology - Week 1 - Class 2Документ14 страницHealth Psychology - Week 1 - Class 2Behroze khalilОценок пока нет
- Personality Disorder PPT ROA FinalДокумент51 страницаPersonality Disorder PPT ROA FinalDat boi50% (4)
- Introduction To Health PsychologyДокумент22 страницыIntroduction To Health PsychologyUm Ar100% (1)
- Short General Health Questionnaire (GHQ 12) : Have You Recently?Документ3 страницыShort General Health Questionnaire (GHQ 12) : Have You Recently?Lydia Yohanna ManzoОценок пока нет
- Stress ScaleДокумент11 страницStress ScaleMona Nath100% (1)
- Facilities For Psycho Social RehabilitationДокумент21 страницаFacilities For Psycho Social RehabilitationRENJULAL93% (15)
- Reply To Pieta MR SinoДокумент9 страницReply To Pieta MR SinoBZ RigerОценок пока нет
- 10 Qualities of An Effective Clinical PsychologistДокумент6 страниц10 Qualities of An Effective Clinical PsychologistShareena M R. Epres100% (2)
- ITC Green Centre: Gurgaon, IndiaДокумент19 страницITC Green Centre: Gurgaon, IndiaAgastya Dasari100% (2)
- Behavior Therapy: Presented By: Saba AhmedДокумент38 страницBehavior Therapy: Presented By: Saba AhmedRana Ahmad GulraizОценок пока нет
- Dollard and Miller: (Psychoanalytic) Learning TheoryДокумент45 страницDollard and Miller: (Psychoanalytic) Learning TheoryFrances LouiseОценок пока нет
- Eastern Perspectives On Positive PsychologyДокумент21 страницаEastern Perspectives On Positive PsychologyAyushi Shakya67% (6)
- Psychophysiological Disorders: Bs 6A+B Urwah AliДокумент29 страницPsychophysiological Disorders: Bs 6A+B Urwah Aliareesha naseerОценок пока нет
- Eastern Perspectives On Positive Psychology: Name: Harshita KapoorДокумент23 страницыEastern Perspectives On Positive Psychology: Name: Harshita KapoorHarshita Kapoor100% (1)
- Charecteristics of A CounsellorДокумент13 страницCharecteristics of A CounsellorVaruni Gupta100% (1)
- Wolberg DefinitionДокумент18 страницWolberg DefinitionSwati ThakurОценок пока нет
- Ivey's PptRead Only)Документ34 страницыIvey's PptRead Only)MAHIMA DASОценок пока нет
- CIS Psych VocationalДокумент12 страницCIS Psych VocationalYogesh Suresh0% (1)
- Wisdom Assessment ScaleДокумент11 страницWisdom Assessment ScaleMehar100% (1)
- Comparing The Major Personality TheoriesДокумент1 страницаComparing The Major Personality TheoriesKate Phebe Bequillo AlahanОценок пока нет
- Historical and Contemporary Views of Abnormal BehaviorДокумент13 страницHistorical and Contemporary Views of Abnormal BehaviorShiela Badiang100% (1)
- Ch-5 Therapeutic Approaches - PPT 3Документ14 страницCh-5 Therapeutic Approaches - PPT 3sayooj tv0% (1)
- Expt 2 - Cognitive Style Inventory - MethodologyДокумент8 страницExpt 2 - Cognitive Style Inventory - Methodologyxijipe1553Оценок пока нет
- Research ProposalДокумент21 страницаResearch ProposalJОценок пока нет
- Mental Health Act PDFДокумент40 страницMental Health Act PDFAnilkumar JaraliОценок пока нет
- Behavioral Analysis PerformaДокумент3 страницыBehavioral Analysis Performashivani singh100% (2)
- MANUAL FOR LEADERSHIP PREFERENCE SCALE (1) - RecognizedДокумент7 страницMANUAL FOR LEADERSHIP PREFERENCE SCALE (1) - RecognizedAshani Aarora0% (1)
- Impression FormationДокумент38 страницImpression Formationpralav0% (1)
- Eastern and Western Perspectives in Positive PsychologyДокумент48 страницEastern and Western Perspectives in Positive PsychologyKritika rastogi100% (2)
- Gerald C. Davison John M. Neale Abnormal Psychology Study Guide John Wiley and Sons 2004Документ243 страницыGerald C. Davison John M. Neale Abnormal Psychology Study Guide John Wiley and Sons 2004Dejana KrstićОценок пока нет
- Scope of Dev. PsychologyДокумент2 страницыScope of Dev. PsychologyEesha TahirОценок пока нет
- Results and Interpretation (NVTI)Документ2 страницыResults and Interpretation (NVTI)Shruti ShrivastavaОценок пока нет
- NOTES Groups HepworthДокумент4 страницыNOTES Groups Hepworthejanis39Оценок пока нет
- 1-The Behavioural Science and HealthДокумент44 страницы1-The Behavioural Science and HealthKhadija Bukhad100% (1)
- CHAPTER 1 LECTURE - An Introduction To Health Psychology FALL 2018Документ57 страницCHAPTER 1 LECTURE - An Introduction To Health Psychology FALL 2018gabiОценок пока нет
- Recovery STAR User Guide PDFДокумент31 страницаRecovery STAR User Guide PDFUm Ar100% (1)
- Ethics Code APA 2017 PDFДокумент20 страницEthics Code APA 2017 PDFinvocatlunaОценок пока нет
- BPS Practice Guidelines (Third Edition)Документ92 страницыBPS Practice Guidelines (Third Edition)Um ArОценок пока нет
- BPS BRoken HeartsДокумент5 страницBPS BRoken HeartsUm ArОценок пока нет
- DAP Draw A Person TestДокумент27 страницDAP Draw A Person TestUm Ar75% (4)
- RaspДокумент15 страницRaspUm ArОценок пока нет
- Officer Like QualitiesДокумент1 страницаOfficer Like QualitiesUm ArОценок пока нет
- Greater Glasgow and ClydeДокумент24 страницыGreater Glasgow and ClydeUm ArОценок пока нет
- S Jozsef Viata in DiosigДокумент52 страницыS Jozsef Viata in Diosigunoradean2Оценок пока нет
- Trần Phương Mai - Literature - Irony in "Letter to a Funeral Parlor" by Lydia DavisДокумент2 страницыTrần Phương Mai - Literature - Irony in "Letter to a Funeral Parlor" by Lydia DavisTrần Phương MaiОценок пока нет
- Effect of Added Sodium Sulphate On Colour Strength and Dye Fixation of Digital Printed Cellulosic FabricsДокумент21 страницаEffect of Added Sodium Sulphate On Colour Strength and Dye Fixation of Digital Printed Cellulosic FabricsSumaiya AltafОценок пока нет
- Reflection On Sumilao CaseДокумент3 страницыReflection On Sumilao CaseGyrsyl Jaisa GuerreroОценок пока нет
- Motion Exhibit 4 - Declaration of Kelley Lynch - 03.16.15 FINALДокумент157 страницMotion Exhibit 4 - Declaration of Kelley Lynch - 03.16.15 FINALOdzer ChenmaОценок пока нет
- Account Statement From 1 Jan 2017 To 30 Jun 2017Документ2 страницыAccount Statement From 1 Jan 2017 To 30 Jun 2017Ujjain mpОценок пока нет
- Pre T&C Checklist (3 Language) - Updated - 2022 DavidДокумент1 страницаPre T&C Checklist (3 Language) - Updated - 2022 Davidmuhammad farisОценок пока нет
- China Daily 20181031Документ24 страницыChina Daily 20181031JackZhangОценок пока нет
- Project TitleДокумент15 страницProject TitleadvikaОценок пока нет
- Account Intel Sample 3Документ28 страницAccount Intel Sample 3CI SamplesОценок пока нет
- Jurnal UlkusДокумент6 страницJurnal UlkusIndri AnggraeniОценок пока нет
- Labor Rules English Noi Quy Bang Tieng Anh PDFДокумент27 страницLabor Rules English Noi Quy Bang Tieng Anh PDFNga NguyenОценок пока нет
- Roman Roads in Southeast Wales Year 3Документ81 страницаRoman Roads in Southeast Wales Year 3The Glamorgan-Gwent Archaeological Trust LtdОценок пока нет
- Psychology and Your Life With Power Learning 3Rd Edition Feldman Test Bank Full Chapter PDFДокумент56 страницPsychology and Your Life With Power Learning 3Rd Edition Feldman Test Bank Full Chapter PDFdiemdac39kgkw100% (9)
- Genomics - FAOДокумент184 страницыGenomics - FAODennis AdjeiОценок пока нет
- Student Worksheet Task 1 - Long Reading: Fanny Blankers-KoenДокумент2 страницыStudent Worksheet Task 1 - Long Reading: Fanny Blankers-KoenDANIELA SIMONELLIОценок пока нет
- Pon Vidyashram Group of Cbse Schools STD 8 SCIENCE NOTES (2020-2021)Документ3 страницыPon Vidyashram Group of Cbse Schools STD 8 SCIENCE NOTES (2020-2021)Bharath Kumar 041Оценок пока нет
- Visual Images of America in The Sixteenth Century: Elaine BrennanДокумент24 страницыVisual Images of America in The Sixteenth Century: Elaine Brennanjoerg_spickerОценок пока нет
- Network Function Virtualization (NFV) : Presented By: Laith AbbasДокумент30 страницNetwork Function Virtualization (NFV) : Presented By: Laith AbbasBaraa EsamОценок пока нет
- K3VG Spare Parts ListДокумент1 страницаK3VG Spare Parts ListMohammed AlryaniОценок пока нет
- Module 1 Facilitator's Guide - Assessing Information NeedsДокумент62 страницыModule 1 Facilitator's Guide - Assessing Information NeedsadkittipongОценок пока нет
- Theo Hermans (Cáp. 3)Документ3 страницыTheo Hermans (Cáp. 3)cookinglike100% (1)
- Conceptual Diagram of Ways To Increase SalesДокумент1 страницаConceptual Diagram of Ways To Increase SalesO6U Pharmacy RecordingsОценок пока нет