Вам также может понравиться
- Example Case StudyДокумент7 страницExample Case StudyTerrena Lyn BlackmanОценок пока нет
- Approach To Pleural EffusionДокумент46 страницApproach To Pleural EffusionBaskoro Tri LaksonoОценок пока нет
- Medical Case of SurgeryДокумент7 страницMedical Case of SurgerysugisweОценок пока нет
- Esophageal Varices: Medication HistoryДокумент4 страницыEsophageal Varices: Medication HistoryNeil Patrick PasuquinОценок пока нет
- Cerebrovascular Disease (Emphasis On CVA)Документ29 страницCerebrovascular Disease (Emphasis On CVA)OlynsieMorrisОценок пока нет
- Dr. Sunatrio - Management Hypovolemic ShockДокумент59 страницDr. Sunatrio - Management Hypovolemic ShockArga Putra SaboeОценок пока нет
- HTN EmergencyДокумент11 страницHTN EmergencyKaran ChhabraОценок пока нет
- Diagnostic SAHДокумент8 страницDiagnostic SAHMohammadAwitОценок пока нет
- 4th Yr. Med Cardio Module Question - Copy-1Документ11 страниц4th Yr. Med Cardio Module Question - Copy-1Sheda BondОценок пока нет
- CPC Acute AppendicitisДокумент57 страницCPC Acute AppendicitisYS Nate100% (1)
- Esophageal Varices Week 4 T2T3Документ37 страницEsophageal Varices Week 4 T2T3liewhuilianОценок пока нет
- Abdominal Blunt TraumaДокумент6 страницAbdominal Blunt TraumaYunes AryoОценок пока нет
- Case Presentation - NSTEMIДокумент18 страницCase Presentation - NSTEMIZОценок пока нет
- Pulmonary EmbolismДокумент46 страницPulmonary EmbolismThevashini Shridaran100% (1)
- Case ReportДокумент38 страницCase ReportDiLa NandaRiОценок пока нет
- Kaposi's SarcomaДокумент6 страницKaposi's SarcomaveremkovichОценок пока нет
- Diabetic NephropathyДокумент6 страницDiabetic NephropathyZulfadliZulfadliОценок пока нет
- Management of OliguriaДокумент14 страницManagement of OliguriaAhmed El-MalkyОценок пока нет
- Cardioembolic Stroke DefinitionДокумент3 страницыCardioembolic Stroke DefinitionJanel TamОценок пока нет
- Acute Renal Failure: Dr. Bobi Ahmad S, S.KPДокумент62 страницыAcute Renal Failure: Dr. Bobi Ahmad S, S.KPdr.Bobi Ahmad Sahid, S.KepОценок пока нет
- Abdominal Aortic Aneurysm and AcuteДокумент8 страницAbdominal Aortic Aneurysm and AcuteKristanto Ayomi Ayomi AriОценок пока нет
- Aneurysmal Subarachnoid Hemorrhage.6Документ19 страницAneurysmal Subarachnoid Hemorrhage.6Aldy Setiawan PutraОценок пока нет
- Electrical BurnsДокумент27 страницElectrical BurnsGautam KalraОценок пока нет
- Asking Your Question (PICO) - NursingДокумент5 страницAsking Your Question (PICO) - NursingBentaigaОценок пока нет
- Ascending CholangitisДокумент7 страницAscending CholangitisAmar HasanОценок пока нет
- Small Bowel ObstructionДокумент2 страницыSmall Bowel ObstructionSrividya PushpalaОценок пока нет
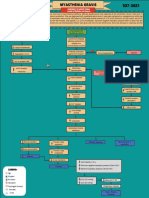
- MYASTHENIA-GRAVIS Concept Map PDFДокумент1 страницаMYASTHENIA-GRAVIS Concept Map PDFAngelo Dela Cruz VillaromanОценок пока нет
- Congestive Heart FailureДокумент14 страницCongestive Heart FailureBella Trix PagdangananОценок пока нет
- Nursing Case Presentation For A Patient With CABG: Subject: Medical Surgical Nursing-IIДокумент10 страницNursing Case Presentation For A Patient With CABG: Subject: Medical Surgical Nursing-IIanamika sharmaОценок пока нет
- How To Define CardiomegalyДокумент2 страницыHow To Define CardiomegalyKjean De Vera MelendezОценок пока нет
- NCP CvaДокумент4 страницыNCP CvaMariquita BuenafeОценок пока нет
- Modified CaseДокумент22 страницыModified CaseAli HawamdeОценок пока нет
- Case Presentation On Ischemic StrokeДокумент55 страницCase Presentation On Ischemic StrokeNisha GuptaОценок пока нет
- Infective Endocarditis Case ReportДокумент40 страницInfective Endocarditis Case Reportliu_owen17100% (1)
- Pathophysiology HeadinjuryДокумент1 страницаPathophysiology HeadinjuryK.b. Dequiña100% (1)
- Clinical Case StudyДокумент5 страницClinical Case Studyv2wish_iОценок пока нет
- Sickle-Cell Anaemia EssayДокумент4 страницыSickle-Cell Anaemia Essayapi-299807117Оценок пока нет
- Vii. Laboratory Results: Hemoglobin 129 MG/DL 140-160 MG/DL LowДокумент2 страницыVii. Laboratory Results: Hemoglobin 129 MG/DL 140-160 MG/DL LowAdrian Dela CruzОценок пока нет
- Approach To QuadriplegiaДокумент4 страницыApproach To QuadriplegiaPraveen BabuОценок пока нет
- REVISED Group4 Congestive Heart FailureДокумент64 страницыREVISED Group4 Congestive Heart FailureNicole Villanueva, BSN - Level 3AОценок пока нет
- Case Study Chest Pain PericarditisДокумент4 страницыCase Study Chest Pain Pericarditisv_vijayakanth765650% (2)
- LA Myxoma Case PresentationДокумент34 страницыLA Myxoma Case PresentationWiwik Puji LestariОценок пока нет
- Good Morning Report!: Nora Switchenko MD R3Документ15 страницGood Morning Report!: Nora Switchenko MD R3Emily EresumaОценок пока нет
- PBL PgamboaДокумент6 страницPBL PgamboaLeanne Princess GamboaОценок пока нет
- Video-Assisted Thoracoscopic Surgery (Vats) in ChildrenДокумент24 страницыVideo-Assisted Thoracoscopic Surgery (Vats) in ChildrenobrankovОценок пока нет
- KARDEX Case 3Документ3 страницыKARDEX Case 3Juviely PremacioОценок пока нет
- Peri TonsilLar AbscessДокумент6 страницPeri TonsilLar Abscessrivan90Оценок пока нет
- Pott Disease 1223292121651385 8Документ54 страницыPott Disease 1223292121651385 8Ismail SalimОценок пока нет
- GE BasavaДокумент21 страницаGE BasavaAmalin PrãdhãñОценок пока нет
- Acute Hypertension-Hypertensive Urgency and Hypertensive EmergencyДокумент13 страницAcute Hypertension-Hypertensive Urgency and Hypertensive EmergencyAmitKumarОценок пока нет
- Adhesive Small Bowel Obstruction: Leslie Kobayashi Trauma Conference 2013Документ56 страницAdhesive Small Bowel Obstruction: Leslie Kobayashi Trauma Conference 2013Ananda RizkiОценок пока нет
- Pericardial EffusionДокумент36 страницPericardial EffusionRizky Amalia Wakano100% (1)
- Introduction - MIДокумент10 страницIntroduction - MIkhimiiiОценок пока нет
- Monro KellieДокумент6 страницMonro Kellievirz23Оценок пока нет
- Pathophysiology: Cholecystitis Non Modifiable Factors Modifiable FactorsДокумент4 страницыPathophysiology: Cholecystitis Non Modifiable Factors Modifiable FactorsLovely DaroleОценок пока нет
- Case Study For Beta Acute Lymphoblastic Leukemia (B-All)Документ15 страницCase Study For Beta Acute Lymphoblastic Leukemia (B-All)Shakira HashimОценок пока нет
- IM AdconДокумент28 страницIM AdconCla SantosОценок пока нет
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Emergency Case Report December, 18 - , 19 2013: Resident On Duty: Dr. Alex Chief On Duty: Galih RahmanДокумент66 страницEmergency Case Report December, 18 - , 19 2013: Resident On Duty: Dr. Alex Chief On Duty: Galih Rahmangalihrahman51Оценок пока нет
- Dislipid, Hipertensi, Crusade, Grace, Kilip ScoreДокумент71 страницаDislipid, Hipertensi, Crusade, Grace, Kilip ScoreWinno Pradana UtomoОценок пока нет
- Systematic ReviewДокумент19 страницSystematic ReviewGery RifanoОценок пока нет
- Daftar Stase Urologi September 2018Документ1 страницаDaftar Stase Urologi September 2018Gery Rifano100% (1)
- Malignant MelanomaДокумент11 страницMalignant MelanomaGery RifanoОценок пока нет
- Pasien Igd Bedah Senin, 28 Agustus 2017 Dr. Jaga: AMS/ WIS/ KBN/ DK/ UDA No. CM Nama Umur/JK Diagnosa Utama Tindakan Sub Bag. KetДокумент2 страницыPasien Igd Bedah Senin, 28 Agustus 2017 Dr. Jaga: AMS/ WIS/ KBN/ DK/ UDA No. CM Nama Umur/JK Diagnosa Utama Tindakan Sub Bag. KetGery RifanoОценок пока нет
- Wiji 15 Juni 17Документ2 страницыWiji 15 Juni 17Gery RifanoОценок пока нет
- Case Report (10.00)Документ11 страницCase Report (10.00)Gery Rifano100% (1)
- The Complete List For The Appraisal of CaseДокумент1 страницаThe Complete List For The Appraisal of CaseGery RifanoОценок пока нет
- Hemostasis & ThrombosisДокумент22 страницыHemostasis & ThrombosisGery RifanoОценок пока нет
- Duty Report 2-3-15Документ3 страницыDuty Report 2-3-15Gery RifanoОценок пока нет
- DL650K9Документ187 страницDL650K9Juan Abraham AjpopОценок пока нет
- Manual Pivot ShuttleДокумент18 страницManual Pivot ShuttleFidel OrtizОценок пока нет
- ZumbaДокумент4 страницыZumbaEdward MirandaОценок пока нет
- Types of EventsДокумент6 страницTypes of EventsBernalyn ManaogОценок пока нет
- Xiiiiiiiiy 9R+Lwqr+K+0 9Zppzpp+Pzpp0 9-+N+-Sn-+0 9+-+-+-Sn-0 9-+P+P+-+0 9+-Zp-+-Zp-0 9P+Qzppzplzp0 9Tr-Vl-+Rmk-0 XiiiiiiiiyДокумент6 страницXiiiiiiiiy 9R+Lwqr+K+0 9Zppzpp+Pzpp0 9-+N+-Sn-+0 9+-+-+-Sn-0 9-+P+P+-+0 9+-Zp-+-Zp-0 9P+Qzppzplzp0 9Tr-Vl-+Rmk-0 XiiiiiiiiyExtraОценок пока нет
- LeversДокумент29 страницLeversShubham KathareОценок пока нет
- Drumeo Edge 1627Документ3 страницыDrumeo Edge 1627Tinavalw DenexwideaОценок пока нет
- Karate Grading - Manual PDFДокумент25 страницKarate Grading - Manual PDFincredibletpОценок пока нет
- Beeman Break Barrel Air Rifle ManualДокумент4 страницыBeeman Break Barrel Air Rifle Manualasrael_grОценок пока нет
- Letter For Parents Drum and Lyre MattersДокумент1 страницаLetter For Parents Drum and Lyre MattersRon RealinОценок пока нет
- Physics Exit 3q1718 .Документ16 страницPhysics Exit 3q1718 .Mikaella Tambis0% (1)
- 8 Week Bulk PDFДокумент19 страниц8 Week Bulk PDFLê Bá Thành PhúОценок пока нет
- DND 5E CharacterSheet FormFillableДокумент3 страницыDND 5E CharacterSheet FormFillableJayson LoulierОценок пока нет
- Harlem Globetrotters - World Tour (USA)Документ12 страницHarlem Globetrotters - World Tour (USA)Tsamis IoannisОценок пока нет
- HikingДокумент2 страницыHikingIanne Violet Yumierre TabañagОценок пока нет
- Just Uploaded To DownloadДокумент4 страницыJust Uploaded To DownloadZachyboiОценок пока нет
- Moir 2017Документ21 страницаMoir 2017Chris Sake100% (1)
- ManifestДокумент43 страницыManifest910611Оценок пока нет
- Nifty Lift - SP 64Документ2 страницыNifty Lift - SP 64ELIZABETH FLETSCHERОценок пока нет
- The Verb Be Evaluation Affirmative FormДокумент2 страницыThe Verb Be Evaluation Affirmative FormMaribel Botero BoteroОценок пока нет
- Recruiting Test General KnowledgeДокумент15 страницRecruiting Test General KnowledgeRelando Bailey83% (175)
- Ballroom DancesДокумент14 страницBallroom DancesLester GarciaОценок пока нет
- 1506a-E88tag3 Electropak Pn3088Документ2 страницы1506a-E88tag3 Electropak Pn3088Md Sh100% (1)
- AWANA Game DirectorДокумент12 страницAWANA Game DirectorFrank TanОценок пока нет
- Motorcyslist Training Course: Student HandbookДокумент98 страницMotorcyslist Training Course: Student Handbookivillacortaav2009Оценок пока нет
- Reliant Motors - WikipediaДокумент51 страницаReliant Motors - WikipediaEndhy Wisnu NovindraОценок пока нет
- Artikel Bahasa Inggris Tentang Kesehatan IДокумент3 страницыArtikel Bahasa Inggris Tentang Kesehatan IRestu Yogi Fahlevi100% (2)
- John Deere 265, 275 & 285 Disc Mowers Diagnostic & Repair Technical Manual TM1795 PDFДокумент11 страницJohn Deere 265, 275 & 285 Disc Mowers Diagnostic & Repair Technical Manual TM1795 PDFEquipment ManualsОценок пока нет
- From Flap Jacks 2 Thick StacksДокумент20 страницFrom Flap Jacks 2 Thick StacksМарсел ДимитровОценок пока нет
- Riva 44' RIVARAMA - Lady MДокумент15 страницRiva 44' RIVARAMA - Lady MskoiperОценок пока нет