Вам также может понравиться
- Preterm LaborДокумент33 страницыPreterm LaborChristian MolinaОценок пока нет
- Abnormal Uterine ActionДокумент27 страницAbnormal Uterine ActionSameer KumarОценок пока нет
- Intrauterine Growth RestrictionДокумент3 страницыIntrauterine Growth RestrictionShofiKhaqulIlmyОценок пока нет
- 4 Pain Management, Theories of Labor Onset, Signs of LaborДокумент31 страница4 Pain Management, Theories of Labor Onset, Signs of Labormamsh KlangОценок пока нет
- PARTOGRAMДокумент36 страницPARTOGRAMNkosinathi ShongweОценок пока нет
- Premature Rupture of MembranesДокумент100 страницPremature Rupture of Membranesztvill100% (1)
- Preconception Care Unit 1Документ42 страницыPreconception Care Unit 1santhiyasandyОценок пока нет
- Intrapartum AssessmentДокумент84 страницыIntrapartum AssessmentAnne Carlie Bucoy RoldanОценок пока нет
- Pre and Post PregnancyДокумент23 страницыPre and Post PregnancyJitendra ChaudharyОценок пока нет
- Intrauterine Fetal DemiseДокумент7 страницIntrauterine Fetal DemiseElaisa Mae Delos SantosОценок пока нет
- Occipito PosteriorpositionДокумент7 страницOccipito PosteriorpositionNishaThakuriОценок пока нет
- Intrauterine Insemination (IUI)Документ6 страницIntrauterine Insemination (IUI)AliaSyafiqaОценок пока нет
- Antepartum Haemorrage (APH) : Dr. Mtumweni, MDДокумент42 страницыAntepartum Haemorrage (APH) : Dr. Mtumweni, MDmarco luenaОценок пока нет
- Family PlanningДокумент13 страницFamily PlanningYana PotОценок пока нет
- Assessment of Fetal Well BeingДокумент29 страницAssessment of Fetal Well Beingmalaika khanОценок пока нет
- High Risk Labor and DeliveryДокумент110 страницHigh Risk Labor and DeliveryWilbert CabanbanОценок пока нет
- Hellp Syndrome: Prepared By: Jamie Niña Faye CДокумент10 страницHellp Syndrome: Prepared By: Jamie Niña Faye CJamie DyОценок пока нет
- PROM SANJIDA FInal 2Документ32 страницыPROM SANJIDA FInal 2Saiful islam RonyОценок пока нет
- 2-Checklist For Pelvis AssessmentДокумент3 страницы2-Checklist For Pelvis AssessmentGazala ParveenОценок пока нет
- Fetal Monitoring CTGДокумент28 страницFetal Monitoring CTGChuah Wei HongОценок пока нет
- Signs and Symptoms of PregnancyДокумент6 страницSigns and Symptoms of Pregnancypppamm100% (1)
- Placental Abruption PresentationДокумент30 страницPlacental Abruption PresentationNafisat AdepojuОценок пока нет
- PARTOGRAMДокумент17 страницPARTOGRAMKrutthivaasa PriyaОценок пока нет
- Placenta Types and GradingДокумент37 страницPlacenta Types and GradingNishant RajОценок пока нет
- 30 - Contracted Pelvis and Cephalopelvic DisproportionДокумент28 страниц30 - Contracted Pelvis and Cephalopelvic Disproportiondr_asaleh93% (14)
- How To Read A CTGДокумент11 страницHow To Read A CTGiwennieОценок пока нет
- Obstetric Emergency - in Primary CareДокумент93 страницыObstetric Emergency - in Primary Careazida90Оценок пока нет
- Fetopelvic DisproportionДокумент6 страницFetopelvic DisproportionPrincess Daulah A. LagasiОценок пока нет
- 3 Problems With The Passenger and Powers of LaborДокумент105 страниц3 Problems With The Passenger and Powers of LaborRaquel M. MendozaОценок пока нет
- Feto Pelvic DisproportionДокумент10 страницFeto Pelvic DisproportionIsrael WoseneОценок пока нет
- Hypertension in Pregnancy-LatestДокумент32 страницыHypertension in Pregnancy-LatestshahiraazОценок пока нет
- Hydatidiform MoleДокумент3 страницыHydatidiform MoleJny SherpaОценок пока нет
- Myoma UteriДокумент21 страницаMyoma UteriLangitBiruОценок пока нет
- Breech PresentationДокумент68 страницBreech PresentationPrathibha Guruguri50% (2)
- 39-Assessment of Fetal Well BeingДокумент34 страницы39-Assessment of Fetal Well Beingdr_asalehОценок пока нет
- Biophysical ProfileДокумент7 страницBiophysical ProfileFloid Tortogo SibbalucaОценок пока нет
- Antepartum Haemorrhage MXДокумент22 страницыAntepartum Haemorrhage MXAmir Hilmi Abd AzizОценок пока нет
- Fetal MonitoringДокумент36 страницFetal MonitoringAshley Etheredge100% (2)
- PartogramДокумент20 страницPartogramKasumba ChandaОценок пока нет
- Placenta Praevia and Placenta AccretaДокумент75 страницPlacenta Praevia and Placenta AccretaNurul Fahmiza TumiranОценок пока нет
- PPROMДокумент63 страницыPPROMSaraMohammedОценок пока нет
- H. Hypertensive Disorders in PregnancyДокумент50 страницH. Hypertensive Disorders in PregnancyRadha ChiombonОценок пока нет
- Cephalopelvic DisproportionДокумент5 страницCephalopelvic DisproportionMaria Donabella OngueОценок пока нет
- 3 (OB Cases)Документ267 страниц3 (OB Cases)Sharyl Plan SarominesОценок пока нет
- Intrauterine Growth RestrictionДокумент7 страницIntrauterine Growth RestrictionNurfazlinaОценок пока нет
- Vasa PraeviaДокумент3 страницыVasa PraeviaAngelica CabututanОценок пока нет
- Nursing Care of Family During Labor and BirthhhДокумент6 страницNursing Care of Family During Labor and BirthhhAudreySalvadorОценок пока нет
- Antepartum HaemorrhageДокумент65 страницAntepartum HaemorrhageAmit RamrattanОценок пока нет
- Abruptio Placenta: Prepared By: Claire Alvarez Ongchua, RNДокумент42 страницыAbruptio Placenta: Prepared By: Claire Alvarez Ongchua, RNclaireaongchua1275100% (2)
- 6 Antepartum Care PDFДокумент24 страницы6 Antepartum Care PDFmohammed farajiОценок пока нет
- Myoma UteriДокумент8 страницMyoma UteriFaraida Arvilla100% (1)
- Uterine FibroidsДокумент25 страницUterine FibroidsMarie Eulie PatinoОценок пока нет
- Apgar ScoreДокумент2 страницыApgar Scorejulialeo100% (3)
- Prelabor Rupture of Membranes (Prom) : By-Aditi Grover Roll No. - 3Документ12 страницPrelabor Rupture of Membranes (Prom) : By-Aditi Grover Roll No. - 3San SiddzОценок пока нет
- Assessment of Fetal Well-BeingДокумент63 страницыAssessment of Fetal Well-BeingArhum Siddiqi100% (1)
- Fetal Morphological and Physiological Development PDFДокумент10 страницFetal Morphological and Physiological Development PDFKim RamosОценок пока нет
- Uterine Fibroids & EndometriosisДокумент82 страницыUterine Fibroids & EndometriosisDuncan Jackson67% (3)
- Multiple Pregnancy 2008Документ61 страницаMultiple Pregnancy 2008Dagnachew kasayeОценок пока нет
- Preterm BirthДокумент11 страницPreterm Birthmendato marcabanОценок пока нет
- Preterm Labor and BirthДокумент55 страницPreterm Labor and BirthEcel AggasidОценок пока нет
- Problem 2 Emergency: Delmy SanjayaДокумент104 страницыProblem 2 Emergency: Delmy SanjayaInd MatthewОценок пока нет
- Problem 3 Emergency: Delmy SanjayaДокумент14 страницProblem 3 Emergency: Delmy SanjayaInd MatthewОценок пока нет
- Pemicu 4: Indriani 405140178Документ51 страницаPemicu 4: Indriani 405140178Ind MatthewОценок пока нет
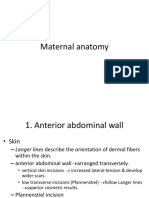
- Maternal AnatomyДокумент60 страницMaternal AnatomyRaraОценок пока нет
- Bromage 1965Документ15 страницBromage 1965Manuel VillasanaОценок пока нет
- Beliefs and Practises Surrounding Postpartum Period Among Malay WomenДокумент9 страницBeliefs and Practises Surrounding Postpartum Period Among Malay WomenBrillo Virla DawnОценок пока нет
- OBSTETRIC NURSING Hand Out UPANG INHOUSE 2022Документ7 страницOBSTETRIC NURSING Hand Out UPANG INHOUSE 2022Mary Ann G. CorsanesОценок пока нет
- Nformation ACK: Specialty Doctor in Anaesthetics and Intensive Care Post Reference 415-MP499-21Документ17 страницNformation ACK: Specialty Doctor in Anaesthetics and Intensive Care Post Reference 415-MP499-21Daniyal AzmatОценок пока нет
- Magnitude and Associated Factors of Respectful Maternity Care in Tirunesh Beijing Hospital, Addis Ababa, Ethiopia, 2021Документ8 страницMagnitude and Associated Factors of Respectful Maternity Care in Tirunesh Beijing Hospital, Addis Ababa, Ethiopia, 2021Amare MisganawОценок пока нет
- Low Cost Solar and Electric Powered Smart Infant IncubatorДокумент23 страницыLow Cost Solar and Electric Powered Smart Infant Incubatora.razakhajiОценок пока нет
- Essential Intrapartum Newborn Care: Prepared byДокумент41 страницаEssential Intrapartum Newborn Care: Prepared byJayrelle D. Safran100% (1)
- TranslateДокумент8 страницTranslateberliananastasya pОценок пока нет
- Low Birth Weight InfantsДокумент5 страницLow Birth Weight Infantserine5995Оценок пока нет
- An Assessment of The Effects of Female Genital Mutilation AmongДокумент57 страницAn Assessment of The Effects of Female Genital Mutilation AmongUsman Ahmad TijjaniОценок пока нет
- Postpartum Care PDFДокумент8 страницPostpartum Care PDF2C- VILLACARLOS, LEONA ROSE M.Оценок пока нет
- Alternative & Complementary Therapy in LabourДокумент14 страницAlternative & Complementary Therapy in Labourhiral mistry87% (15)
- Contracted Pelvis by KABERA ReneДокумент14 страницContracted Pelvis by KABERA ReneKABERA RENEОценок пока нет
- Situation Analysis of Community Midwives ' Training in SindhДокумент107 страницSituation Analysis of Community Midwives ' Training in Sindhmidwifepak100% (1)
- Ncma217 Lec MidtermДокумент21 страницаNcma217 Lec Midtermcaitie miracleОценок пока нет
- Almonte HistoryДокумент3 страницыAlmonte HistoryAngelo ErispeОценок пока нет
- 10 The Role of Routine Cervical Length Screening in Selected High - and Low-Risk Women For Preterm Birth PreventionДокумент6 страниц10 The Role of Routine Cervical Length Screening in Selected High - and Low-Risk Women For Preterm Birth PreventionWailea Faye SalvaОценок пока нет
- DOLE Department Order On Night WorkersДокумент5 страницDOLE Department Order On Night Workersgoannamarie7814100% (1)
- Ob Part 2Документ7 страницOb Part 2gmik02Оценок пока нет
- Predictors of Traumatic Birth Experience Among A Group of Iranian Primipara Women: A Cross Sectional StudyДокумент9 страницPredictors of Traumatic Birth Experience Among A Group of Iranian Primipara Women: A Cross Sectional Studycocoon cocoonyОценок пока нет
- OB-GynMCQ S BlueprintДокумент20 страницOB-GynMCQ S BlueprintDivine Sangutan100% (1)
- Breech PresentationДокумент27 страницBreech PresentationNurkamilawati AristaОценок пока нет
- Procedures Used in The Management of DystociaДокумент17 страницProcedures Used in The Management of DystociaRavi RokkamОценок пока нет
- Assessment of Fetal WellbeingДокумент24 страницыAssessment of Fetal WellbeingMukesh ThakurОценок пока нет
- 20 - Obstetrical Analgesia and AnesthesiaДокумент9 страниц20 - Obstetrical Analgesia and AnesthesiaGen XОценок пока нет
- Radu Cinamar - Peter Moon - Transylvanian Sunrise (2003)Документ282 страницыRadu Cinamar - Peter Moon - Transylvanian Sunrise (2003)lennardvandergraafОценок пока нет
- CPG Abnormal Labor and Delivery PDFДокумент29 страницCPG Abnormal Labor and Delivery PDFKarl Jimenez Separa100% (2)
- Mother FatherДокумент10 страницMother FatherAnonymousTargetОценок пока нет
- Obstetric Neurological Injuries: ReviewДокумент8 страницObstetric Neurological Injuries: Reviewaish25Оценок пока нет
- Bakri BalloonДокумент3 страницыBakri BalloonancoursОценок пока нет