Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Method Statement (RC Slab)Документ3 страницыMethod Statement (RC Slab)group2sd131486% (7)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Exercises - Fluid MechanicsДокумент3 страницыExercises - Fluid MechanicsgemnikkicОценок пока нет
- 6 Kuliah Liver CirrhosisДокумент55 страниц6 Kuliah Liver CirrhosisAnonymous vUEDx8100% (1)
- For PDFДокумент1 страницаFor PDFArgia AnjaniОценок пока нет
- Tugas PenelitianДокумент2 страницыTugas PenelitianArgia AnjaniОценок пока нет
- The Effect of Topically Applied Aspirin On Localizezd Circumscribed NeurodermatitisДокумент15 страницThe Effect of Topically Applied Aspirin On Localizezd Circumscribed NeurodermatitisArgia AnjaniОценок пока нет
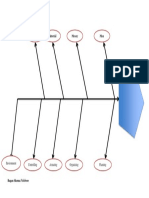
- Method Material Money Man: Bagan Skema FishboneДокумент1 страницаMethod Material Money Man: Bagan Skema FishboneArgia AnjaniОценок пока нет
- Chapter 2 and 3 ImmunologyДокумент16 страницChapter 2 and 3 ImmunologyRevathyОценок пока нет
- Enviroline 2405: Hybrid EpoxyДокумент4 страницыEnviroline 2405: Hybrid EpoxyMuthuKumarОценок пока нет
- Big 9 Master SoalДокумент6 страницBig 9 Master Soallilik masrukhahОценок пока нет
- Laboratory Cold ChainДокумент22 страницыLaboratory Cold ChainEmiОценок пока нет
- BMJ 40 13Документ8 страницBMJ 40 13Alvin JiwonoОценок пока нет
- NRF Nano EthicsДокумент18 страницNRF Nano Ethicsfelipe de jesus juarez torresОценок пока нет
- Rooftop Rain Water Harvesting in An Educational CampusДокумент9 страницRooftop Rain Water Harvesting in An Educational CampusAkshay BoratiОценок пока нет
- GEC - ReviewerДокумент23 страницыGEC - ReviewerGlycel BagabagonОценок пока нет
- Ds0h Ufaa68 ProposalДокумент11 страницDs0h Ufaa68 Proposaledward baskaraОценок пока нет
- ISO - TR - 15608 - 2017 (En) - Pipe Grouping SystemsДокумент12 страницISO - TR - 15608 - 2017 (En) - Pipe Grouping SystemsTeodor ProdanОценок пока нет
- Narrative Report On Weekly Accomplishments: Department of EducationДокумент2 страницыNarrative Report On Weekly Accomplishments: Department of Educationisha mariano100% (1)
- Cadorna, Chesca L. - NCPДокумент2 страницыCadorna, Chesca L. - NCPCadorna Chesca LoboОценок пока нет
- Analysis of Pure Copper - A Comparison of Analytical MethodsДокумент12 страницAnalysis of Pure Copper - A Comparison of Analytical Methodsban bekasОценок пока нет
- Epo-Fix Plus: High-Performance Epoxy Chemical AnchorДокумент3 страницыEpo-Fix Plus: High-Performance Epoxy Chemical Anchormilivoj ilibasicОценок пока нет
- Assignment - Lab Accidents and PrecautionsДокумент6 страницAssignment - Lab Accidents and PrecautionsAnchu AvinashОценок пока нет
- Inlet Manifold Pressure - Test: Testing and AdjustingДокумент2 страницыInlet Manifold Pressure - Test: Testing and AdjustingAbdoulaye Boua BERTHEОценок пока нет
- Those With MoonДокумент1 страницаThose With MoonRosee AldamaОценок пока нет
- Mainstreaming Gad Budget in The SDPДокумент14 страницMainstreaming Gad Budget in The SDPprecillaugartehalagoОценок пока нет
- Cargador de BateríaДокумент34 страницыCargador de BateríaBenОценок пока нет
- Weld Metal Overlay & CladdingДокумент2 страницыWeld Metal Overlay & CladdingbobyОценок пока нет
- Parche CRP 65 - Ficha Técnica - en InglesДокумент2 страницыParche CRP 65 - Ficha Técnica - en IngleserwinvillarОценок пока нет
- Conference Version of SB 1Документ486 страницConference Version of SB 1Paul MastersОценок пока нет
- DT 2107Документ1 страницаDT 2107Richard PeriyanayagamОценок пока нет
- Neuro M Summary NotesДокумент4 страницыNeuro M Summary NotesNishikaОценок пока нет
- Sample SWMSДокумент4 страницыSample SWMSJuma KavesuОценок пока нет
- Characteristics of Testable HypothesesДокумент30 страницCharacteristics of Testable HypothesesMarivic Diano67% (3)
- Recruitement Process - Siemens - Sneha Waman Kadam S200030047 PDFДокумент7 страницRecruitement Process - Siemens - Sneha Waman Kadam S200030047 PDFSneha KadamОценок пока нет