Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Health Questionnaire TemplateДокумент2 страницыHealth Questionnaire TemplateBaxwal AxmedОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- 9c5ff54e-92aa-4393-8350-218e91c128d2Документ6 страниц9c5ff54e-92aa-4393-8350-218e91c128d2Zarbakht AliОценок пока нет
- Mycobacterial Infections Hcu Aug 2016 PDFДокумент5 страницMycobacterial Infections Hcu Aug 2016 PDFumarОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Cognitive Rehab For StrokeДокумент19 страницCognitive Rehab For StrokeAisyah IcahОценок пока нет
- Working With Whiplash, Part I (Myofascial Techniques)Документ5 страницWorking With Whiplash, Part I (Myofascial Techniques)Advanced-Trainings.com100% (4)
- Pharma Prelim ExamДокумент6 страницPharma Prelim ExamMelody DoriaОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Exercise of Body MechanicsДокумент4 страницыExercise of Body Mechanicslostloved7Оценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Blood Cells LabДокумент7 страницBlood Cells LabKameron WardОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Assessment of Pregnant Woman 2023Документ2 страницыAssessment of Pregnant Woman 2023ysohidalgo13Оценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Transplantation: Treatment Methods For Kidney FailureДокумент28 страницTransplantation: Treatment Methods For Kidney FailurecopiimeiОценок пока нет
- Toronto Cataract ConferenceДокумент6 страницToronto Cataract ConferenceDee Margaux SantiagoОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Case Proforma Final, SurgeryДокумент37 страницCase Proforma Final, SurgeryDiwakesh C B100% (4)
- Cardioplegia Types and Methods of AdministrationДокумент59 страницCardioplegia Types and Methods of Administrationgovind_soni_150% (2)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Phaseolus VulgarisДокумент25 страницPhaseolus VulgarisMueen mohsinОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Drug Study CeelinДокумент2 страницыDrug Study Ceelinanonymoustiger100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Asthma: Kaps PrepДокумент21 страницаAsthma: Kaps PrepImee TingzonОценок пока нет
- 2.early Pregnancy and BleedingДокумент79 страниц2.early Pregnancy and BleedingjosephОценок пока нет
- Zimmer Biomet ANZ Fellowship Directory 2019Документ22 страницыZimmer Biomet ANZ Fellowship Directory 2019FahadОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- GGT enДокумент2 страницыGGT enKaoueche OmarОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- VACCINESДокумент8 страницVACCINESzilikajainОценок пока нет
- Parasitology - TrematodesДокумент16 страницParasitology - TrematodesMarlex SuanОценок пока нет
- UNEP Directory March 2021Документ34 страницыUNEP Directory March 2021Perera KusalОценок пока нет
- ESSAYДокумент2 страницыESSAYBokОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
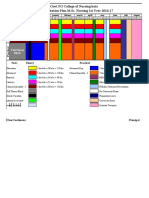
- 10.master Rotation Plan M. Sc. Nursing 1st YearДокумент4 страницы10.master Rotation Plan M. Sc. Nursing 1st YearNaresh JeengarОценок пока нет
- Grade 6: The Heart and Circulatory SystemДокумент18 страницGrade 6: The Heart and Circulatory SystemEstanislao Villanueva ElemОценок пока нет
- Kuliah Hemoglobinopati - Uin Syarif Hidayatullah - Mei 2010Документ35 страницKuliah Hemoglobinopati - Uin Syarif Hidayatullah - Mei 2010Nurraisya MutiyaniОценок пока нет
- Moxibustion OutputДокумент2 страницыMoxibustion OutputJhon Carlo TegioОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Drug Study - HydrocortisoneДокумент5 страницDrug Study - HydrocortisoneryanОценок пока нет
- Angiodroid The CO2 Injector - VascupediaДокумент8 страницAngiodroid The CO2 Injector - VascupediaArnaud TORNIERОценок пока нет
- Admission Booking Form, Rev. 8Документ1 страницаAdmission Booking Form, Rev. 8Eking InОценок пока нет