Вам также может понравиться
- Narrative Report: Division of Surigao Del SurДокумент2 страницыNarrative Report: Division of Surigao Del SurMaria Rose Tariga Aquino83% (6)
- The Flight To Intimacy - The Flight From IntimacyДокумент5 страницThe Flight To Intimacy - The Flight From IntimacyRatna Bhūṣaṇa Bhūṣaṇā Dāsa100% (2)
- Organisational Behavior Lessons From Movie - Pursuit of HappinessДокумент21 страницаOrganisational Behavior Lessons From Movie - Pursuit of HappinessCHITTARANJAN SHETTYОценок пока нет
- Art of AppreciationДокумент7 страницArt of AppreciationevkaevkaОценок пока нет
- Robert Daniel School Counselor Cover LetterДокумент1 страницаRobert Daniel School Counselor Cover Letterapi-512429614Оценок пока нет
- Lodge - Analysis and Interpretation of The Realist TextДокумент19 страницLodge - Analysis and Interpretation of The Realist TextHumano Ser0% (1)
- One Day Workshop Agenda TemplateДокумент11 страницOne Day Workshop Agenda Templatemanjit yadavОценок пока нет
- Lesson Plan - Piropos: Outcomes From Alberta Program of Studies Overview of LessonДокумент2 страницыLesson Plan - Piropos: Outcomes From Alberta Program of Studies Overview of Lessonapi-300398649Оценок пока нет
- Princess Bride AnalysisДокумент3 страницыPrincess Bride Analysisapi-287028218100% (2)
- Japan Negotiation StylesДокумент3 страницыJapan Negotiation StylesFarzana RosliОценок пока нет
- Theory of LoveДокумент6 страницTheory of LoveShaurya KapoorОценок пока нет
- Interpersonal Communications Chapter 3Документ9 страницInterpersonal Communications Chapter 3randomscribduser2012Оценок пока нет
- Unit 2 RelationshipДокумент26 страницUnit 2 Relationshippck1004Оценок пока нет
- Leadership and Management PDFДокумент2 страницыLeadership and Management PDFmnmrzn100% (1)
- 3 Foundations of Healthy Relationships-1Документ42 страницы3 Foundations of Healthy Relationships-1Anurag Soni100% (1)
- 13 How Are Attachments DevelopedДокумент13 страниц13 How Are Attachments DevelopedJay L ParallagОценок пока нет
- Army Leadership (Be, Know, Do)Документ30 страницArmy Leadership (Be, Know, Do)risto420Оценок пока нет
- Emotional Development & Attachment (AMADO M. CADIONG MAED-PED) ESSU - BRORNGAN CITYДокумент39 страницEmotional Development & Attachment (AMADO M. CADIONG MAED-PED) ESSU - BRORNGAN CITYAmado M CadiongОценок пока нет
- Honesty and Personal RelationshipДокумент43 страницыHonesty and Personal RelationshipChristopher CorozaОценок пока нет
- Romantic Relationships in Light of AttacДокумент10 страницRomantic Relationships in Light of Attacshamaila2405Оценок пока нет
- Servant LeadershipДокумент6 страницServant LeadershipJenny MattsonОценок пока нет
- JOHN DEWEY'S THEORY OF INQUIRY AN INTERPRETATION OF A Classic American To LogicДокумент104 страницыJOHN DEWEY'S THEORY OF INQUIRY AN INTERPRETATION OF A Classic American To LogicMuneerh AlhazzaniОценок пока нет
- The Abrasive PersonalityДокумент7 страницThe Abrasive PersonalityArmando Duarte GalánОценок пока нет
- The 4 Inmate Personality TypesДокумент7 страницThe 4 Inmate Personality TypesLeahu BeatriceОценок пока нет
- Attachment Styles: An Evolving Taxonomy of Evolutionarily Adaptive and Maladaptive Affectional BondsДокумент2 страницыAttachment Styles: An Evolving Taxonomy of Evolutionarily Adaptive and Maladaptive Affectional BondsTubocurareОценок пока нет
- Romantic AttachementДокумент174 страницыRomantic AttachementJowana Abou shakraОценок пока нет
- Growing Up With Parental Alcohol Abuse, Exposure To Childhood Abuse, Neglect, and Household DysfunctionДокумент14 страницGrowing Up With Parental Alcohol Abuse, Exposure To Childhood Abuse, Neglect, and Household DysfunctionAndreea PalОценок пока нет
- Adler CH1Документ15 страницAdler CH1Tesla DietzОценок пока нет
- Social Psychology: David Myers 11e Attraction and Intimacy: Liking and Loving OthersДокумент25 страницSocial Psychology: David Myers 11e Attraction and Intimacy: Liking and Loving OthersOlivia S. AgustinОценок пока нет
- The Quick Guide To Admissions ResumesДокумент14 страницThe Quick Guide To Admissions ResumesHafsa JalalОценок пока нет
- Personal Relationships of Adolescents 1Документ41 страницаPersonal Relationships of Adolescents 1Bea Valerie GrislerОценок пока нет
- Infidelity in RelationshipsДокумент3 страницыInfidelity in RelationshipsYadira Estrada GuevaraОценок пока нет
- Love - Bondage or Liberation - A Psychological Exploration of The Meaning, Values and Dangers of Falling in Love PDFДокумент209 страницLove - Bondage or Liberation - A Psychological Exploration of The Meaning, Values and Dangers of Falling in Love PDFPurnendra SinghОценок пока нет
- Army Leadership and CounselingДокумент12 страницArmy Leadership and CounselingMathematicus MathematicaОценок пока нет
- Global Ethics: All About ArgumentsДокумент8 страницGlobal Ethics: All About ArgumentsΘεόφραστοςОценок пока нет
- American History X AnalysisДокумент2 страницыAmerican History X AnalysisrFernandez369Оценок пока нет
- Worksheet Chapter 4Документ4 страницыWorksheet Chapter 4Boros Meh Meh100% (1)
- Why Narcissists Are Unwilling To Apologize The Role of Empathy and Guilt-Leunissen2017Документ19 страницWhy Narcissists Are Unwilling To Apologize The Role of Empathy and Guilt-Leunissen2017Jacobo riquelme100% (1)
- The Self With OthersДокумент61 страницаThe Self With OthersJohnny Ortega Sy Reyes IIОценок пока нет
- Family Violence: Explanations and Evidence-Based Clinical PracticeОт EverandFamily Violence: Explanations and Evidence-Based Clinical PracticeОценок пока нет
- Appendix C List of Character TraitsДокумент3 страницыAppendix C List of Character Traitsmilkymilky9876Оценок пока нет
- Communications Exam IIДокумент8 страницCommunications Exam IILee Alexander PrestonОценок пока нет
- On Being Just Friends' The Frequency and Impact of Sexual Activity in Crosssex FriendshipsДокумент18 страницOn Being Just Friends' The Frequency and Impact of Sexual Activity in Crosssex FriendshipsRoxana SerghieОценок пока нет
- Devdeep Roy Chowdhury, M.SC, M.Phil Clinical PsychologistДокумент12 страницDevdeep Roy Chowdhury, M.SC, M.Phil Clinical PsychologistDevdeep Roy ChowdhuryОценок пока нет
- The Effect of AttachmentДокумент11 страницThe Effect of AttachmentȘtefan Petre100% (1)
- Afifi and Reichert 1996Документ12 страницAfifi and Reichert 1996Farva MoidОценок пока нет
- Personality and Personal EffectivenessДокумент29 страницPersonality and Personal Effectivenessachannoji100% (1)
- Developing A Leadership PhilosophyДокумент7 страницDeveloping A Leadership PhilosophysoniyarahateОценок пока нет
- Stella's Girl: The Autobiography of Captain Evelyn Decker, a World War Ii and Korean War VeteranОт EverandStella's Girl: The Autobiography of Captain Evelyn Decker, a World War Ii and Korean War VeteranОценок пока нет
- AttachmentДокумент30 страницAttachmentJulián Alberto Muñoz FigueroaОценок пока нет
- Parent Child Bed SharingДокумент24 страницыParent Child Bed SharingquinhoxОценок пока нет
- Emotional Intelligence and Critical ThinkingДокумент17 страницEmotional Intelligence and Critical ThinkingRichard WarrenОценок пока нет
- Week 11 - The Beauty of Conflict - ARGДокумент3 страницыWeek 11 - The Beauty of Conflict - ARGginger pampuОценок пока нет
- Emotional and Social SelfДокумент18 страницEmotional and Social Selfkhatrinakhate04Оценок пока нет
- Cognitive TherapyДокумент18 страницCognitive TherapyHaysheryl Vallejo SalamancaОценок пока нет
- Biopsychosocial Assessment Format2Документ3 страницыBiopsychosocial Assessment Format2Hassan MaqsoodОценок пока нет
- Codes of Gender Study GuideДокумент15 страницCodes of Gender Study Guidezinkblink100% (1)
- Adult LearnersДокумент23 страницыAdult LearnersMark BautistaОценок пока нет
- Emotionnal Intelligence NДокумент26 страницEmotionnal Intelligence Nrabin neupaneОценок пока нет
- Lying: To Lie Is To Deliver A False Statement To Another Person Which The Speaking Person Know Is Not The Whole TruthДокумент14 страницLying: To Lie Is To Deliver A False Statement To Another Person Which The Speaking Person Know Is Not The Whole TruthjhannaОценок пока нет
- Attendance Ict FebruaryДокумент9 страницAttendance Ict FebruaryjeromeОценок пока нет
- Integer Damath Printable ChipsДокумент1 страницаInteger Damath Printable ChipsjeromeОценок пока нет
- Computer VirusДокумент25 страницComputer VirusjeromeОценок пока нет
- Looooooooong Quizzzzzzzzz Tle 10Документ12 страницLooooooooong Quizzzzzzzzz Tle 10jeromeОценок пока нет
- Looooooooong QuizzzzzzzzzДокумент6 страницLooooooooong QuizzzzzzzzzjeromeОценок пока нет
- How To Make A Damath Board and ChipsДокумент4 страницыHow To Make A Damath Board and Chipsjerome100% (1)
- Attendance Ict FebruaryДокумент9 страницAttendance Ict FebruaryjeromeОценок пока нет
- Long Quiz: Quarter 3 03-22-23 #PurplewednesdaysДокумент33 страницыLong Quiz: Quarter 3 03-22-23 #PurplewednesdaysjeromeОценок пока нет
- Tle-Css Q3Документ31 страницаTle-Css Q3jeromeОценок пока нет
- Vawc 2021 Iec MaterialДокумент4 страницыVawc 2021 Iec MaterialjeromeОценок пока нет
- 3rd Periodical Examination Math 7 RegulaДокумент4 страницы3rd Periodical Examination Math 7 RegulajeromeОценок пока нет
- Tle Ict 10 q4 Inc Week 5 8f 2Документ25 страницTle Ict 10 q4 Inc Week 5 8f 2jeromeОценок пока нет
- Exam FormatДокумент1 страницаExam FormatjeromeОценок пока нет
- ARPresentation Template 1Документ11 страницARPresentation Template 1jeromeОценок пока нет
- Municipality Name Results of The 2019 Math Festival ISMC Municipal Level Registration TemplateДокумент11 страницMunicipality Name Results of The 2019 Math Festival ISMC Municipal Level Registration TemplatejeromeОценок пока нет
- DLL Chs 2nd Quarter Week 1Документ3 страницыDLL Chs 2nd Quarter Week 1jeromeОценок пока нет
- Student Template 16x9Документ5 страницStudent Template 16x9jeromeОценок пока нет
- 2016 Learner Individual Registration FormДокумент1 страница2016 Learner Individual Registration FormErnilyn Ligan100% (3)
- Standard and Performance Indicator Map With Answer Key 2007 Grade 7 MathematicsДокумент2 страницыStandard and Performance Indicator Map With Answer Key 2007 Grade 7 MathematicsjeromeОценок пока нет
- Maths Template 16x9Документ5 страницMaths Template 16x9jeromeОценок пока нет
- AR Table and Graph FormatДокумент2 страницыAR Table and Graph FormatjeromeОценок пока нет
- Mathematics Tests:, Grades, andДокумент32 страницыMathematics Tests:, Grades, andjeromeОценок пока нет
- Title THE EFFECTS OF STRATEGIC INTERVENTДокумент10 страницTitle THE EFFECTS OF STRATEGIC INTERVENTPaul Mark DizonОценок пока нет
- Mathematics Test: Book 2Документ16 страницMathematics Test: Book 2misterreidОценок пока нет
- Standard and Performance Indicator Map With Answer Key 2007 Grade 7 MathematicsДокумент2 страницыStandard and Performance Indicator Map With Answer Key 2007 Grade 7 MathematicsjeromeОценок пока нет
- Book 2Документ16 страницBook 2jeromeОценок пока нет
- Ipcrf New 2019 For Guro AkoДокумент99 страницIpcrf New 2019 For Guro AkoNorjainaОценок пока нет
- Mathematics Test: Book 2Документ16 страницMathematics Test: Book 2jeromeОценок пока нет
- Book 2Документ16 страницBook 2jeromeОценок пока нет
- Sample Book 1Документ22 страницыSample Book 1jeromeОценок пока нет
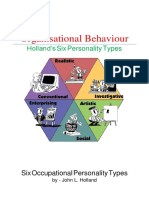
- Organisational Behaviour: Holland's Six Personality TypesДокумент5 страницOrganisational Behaviour: Holland's Six Personality TypesKarina PoОценок пока нет
- Running Head: Analysis of A Developmental Case Study 1Документ4 страницыRunning Head: Analysis of A Developmental Case Study 1alexОценок пока нет
- Consumer Behaviour LorealДокумент48 страницConsumer Behaviour LorealPiyush BaidОценок пока нет
- Nurse - Client RelationshipДокумент88 страницNurse - Client RelationshipShara SampangОценок пока нет
- Communication ModelsДокумент15 страницCommunication ModelsGourav Batheja classesОценок пока нет
- Nursing Leadership Philosophy PaperДокумент6 страницNursing Leadership Philosophy Paperapi-355764752100% (1)
- HumanismДокумент2 страницыHumanismArianne Grace FloresОценок пока нет
- Chapter 2.4 PDFДокумент20 страницChapter 2.4 PDFmahesh_khebadeОценок пока нет
- Glasser's "Reality Therapy" ModelДокумент27 страницGlasser's "Reality Therapy" ModelNieysa AdyОценок пока нет
- Learning Environment and Teaching StrategiesДокумент3 страницыLearning Environment and Teaching StrategiesJovie MasongsongОценок пока нет
- PsychodynamicДокумент12 страницPsychodynamicLindsey MillerОценок пока нет
- Individual Memo of LeadershipДокумент5 страницIndividual Memo of LeadershipDivya SmoozОценок пока нет
- Theoretical Framework and Hypothesis DevelopmentДокумент19 страницTheoretical Framework and Hypothesis Developmentgaturora67% (6)
- Behavioural Based Interview QuestionsДокумент2 страницыBehavioural Based Interview QuestionsspidersurverОценок пока нет
- Develop Your Interpersonal SkillsДокумент41 страницаDevelop Your Interpersonal SkillsChangpu YnchngОценок пока нет
- Psychiatric Nursing Exam 14 NLE PreДокумент4 страницыPsychiatric Nursing Exam 14 NLE Prelovely_omegaОценок пока нет
- Human Communication: What and WhyДокумент20 страницHuman Communication: What and WhyRogelio ZepedaОценок пока нет
- Assignment 1 SaikolojiДокумент7 страницAssignment 1 SaikolojiGIBSONОценок пока нет
- T T T Team Eam Eam Eam Workshop Design Workshop Design Workshop Design Workshop DesignДокумент9 страницT T T Team Eam Eam Eam Workshop Design Workshop Design Workshop Design Workshop DesignJeanny Salamanca De GuzmanОценок пока нет
- Immensely Social: Mindful Monday: Jack Canfield-Activate The Law of AttractionДокумент8 страницImmensely Social: Mindful Monday: Jack Canfield-Activate The Law of AttractionswarajchaОценок пока нет
- Jensen Shoes Case Study - Hrm5001: Group MembersДокумент4 страницыJensen Shoes Case Study - Hrm5001: Group MembersSai Sujith PoosarlaОценок пока нет
- Mabini Colleges Inc. Graduate School: Vision MissionДокумент4 страницыMabini Colleges Inc. Graduate School: Vision MissionLenielynBisoОценок пока нет
- Student Centered Learning For ESLДокумент24 страницыStudent Centered Learning For ESLJeff AskewjОценок пока нет
- Niosh Occupational StressДокумент19 страницNiosh Occupational Stressrachel kingОценок пока нет