Вам также может понравиться
- Kegawatan Jantung - MeДокумент41 страницаKegawatan Jantung - MeNam Min BinОценок пока нет
- Immunopatologi Sepsis - DR Nur Farhanah SPPD K-PTIДокумент29 страницImmunopatologi Sepsis - DR Nur Farhanah SPPD K-PTIanita tri hastutiОценок пока нет
- Stemi Acute Coronary Syndrome: Dr. Muh A Sungkar, SPPD, SPJP, KKVДокумент35 страницStemi Acute Coronary Syndrome: Dr. Muh A Sungkar, SPPD, SPJP, KKVCoass BonamОценок пока нет
- Treating Dengue Shock Syndrome with Fluid ManagementДокумент29 страницTreating Dengue Shock Syndrome with Fluid ManagementTugas HeinzОценок пока нет
- Testicular Torsion GuideДокумент14 страницTesticular Torsion GuideRizkiYudaPurnomoОценок пока нет
- Gasem MH HANTA Salatiga 2019Документ43 страницыGasem MH HANTA Salatiga 2019ChristianОценок пока нет
- HFpEF MeДокумент28 страницHFpEF MeRidwan YasinОценок пока нет
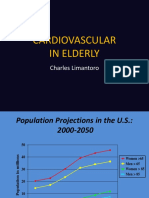
- Cardiovascular in Elderly NewДокумент23 страницыCardiovascular in Elderly NewVania OktavianiОценок пока нет
- Fever of Unknown OriginДокумент33 страницыFever of Unknown OriginRanjit Kumar ShahОценок пока нет
- SS II.1.1 Update On Typhoid Management - Dr. Adityo Susilo, SpPD-KPTI PDFДокумент34 страницыSS II.1.1 Update On Typhoid Management - Dr. Adityo Susilo, SpPD-KPTI PDFWisnu Yudho HОценок пока нет
- Emerging, Re-emerging Diseases and NTDs in IndonesiaДокумент32 страницыEmerging, Re-emerging Diseases and NTDs in IndonesiaMelia100% (1)
- NEUROGENIC BLADDER Nov 2021Документ100 страницNEUROGENIC BLADDER Nov 2021Ranjit SharmaОценок пока нет
- Approach To The Adult With EpistaxisДокумент18 страницApproach To The Adult With EpistaxisTP RMad100% (1)
- Investigation Diagnosis ManagementДокумент35 страницInvestigation Diagnosis ManagementDo Minh TungОценок пока нет
- Concept MapДокумент4 страницыConcept MapDud AccОценок пока нет
- Ventikular Septal Defect FixДокумент18 страницVentikular Septal Defect FixPutri Sari DewiОценок пока нет
- Heparin Induced ThrombocytopeniaДокумент29 страницHeparin Induced Thrombocytopeniahari krishna100% (6)
- CASE REPORT PiopneumothoraksДокумент9 страницCASE REPORT PiopneumothoraksAmriansyah PranowoОценок пока нет
- CVP Guided Deresuscitation in Managing Overload in Icu PDFДокумент57 страницCVP Guided Deresuscitation in Managing Overload in Icu PDFJonathan Hamm100% (1)
- EMPYEMAДокумент27 страницEMPYEMAMark Bin S. DilangalenОценок пока нет
- Dengue Hemorrhagic Fever (DHF)Документ9 страницDengue Hemorrhagic Fever (DHF)Muhamad Hilal Rizki KusumaОценок пока нет
- SEPSIS Kuliah Prof Herdiman (S1) RevДокумент41 страницаSEPSIS Kuliah Prof Herdiman (S1) RevSianipar Mangara Wahyu CharrosОценок пока нет
- AutismДокумент10 страницAutismapi-314229616100% (1)
- Management of Infective EndocarditisДокумент14 страницManagement of Infective Endocarditismhafzam2020Оценок пока нет
- Appendicitis SchwartzДокумент47 страницAppendicitis SchwartzJuan Carlos SantamariaОценок пока нет
- Tetanus: Basic Information DiagnosisДокумент2 страницыTetanus: Basic Information DiagnosisAndi Muslih RijalОценок пока нет
- Cardiorespiratory ArrestДокумент51 страницаCardiorespiratory ArrestIrham KhairiОценок пока нет
- Valvular Heart DiseaseДокумент62 страницыValvular Heart DiseaseRidhaОценок пока нет
- Kuliah Thrombosis 2015 NNДокумент39 страницKuliah Thrombosis 2015 NNBeladiena Citra SiregarОценок пока нет
- Penile Cancer 2010Документ28 страницPenile Cancer 2010raghavagummadiОценок пока нет
- Everything You Need to Know About DyspneaДокумент34 страницыEverything You Need to Know About DyspneaAlvin BrilianОценок пока нет
- Hepatocellular Carcinoma: Rahela Šafarić, 4th Year 2021/2022Документ15 страницHepatocellular Carcinoma: Rahela Šafarić, 4th Year 2021/2022Rahela WaleОценок пока нет
- Pathophysiology Diagram of Kawasaki Disease: Precipitating Factors: Predisposing FactorsДокумент2 страницыPathophysiology Diagram of Kawasaki Disease: Precipitating Factors: Predisposing FactorsAb Staholic Boii100% (1)
- EdemaДокумент27 страницEdemarapadilОценок пока нет
- Assessment and Initial Management Trauma PatientДокумент69 страницAssessment and Initial Management Trauma PatientdrpagrawОценок пока нет
- Strengthening Philippine Disaster Risk Reduction ActДокумент1 страницаStrengthening Philippine Disaster Risk Reduction Actkleford BateОценок пока нет
- Generic Name Brand Name Drug Class Mechanism of Action StructureДокумент4 страницыGeneric Name Brand Name Drug Class Mechanism of Action StructurenoelkiddoОценок пока нет
- Management of ACS Complicated With Acute Heart Failure DR BudianaДокумент27 страницManagement of ACS Complicated With Acute Heart Failure DR BudianaLuh Leni AriniОценок пока нет
- Understanding NystagmusДокумент14 страницUnderstanding NystagmusJefferson CaesarioОценок пока нет
- Abdominal Compartment SyndromeДокумент7 страницAbdominal Compartment Syndromemezgebu alemnehОценок пока нет
- CASE REPORT GinekomastiaДокумент28 страницCASE REPORT GinekomastialaurahardiniОценок пока нет
- 06prof. Riwanto-Abdominal Compartment SyndromeДокумент41 страница06prof. Riwanto-Abdominal Compartment SyndromeTanujaa Venugopal100% (1)
- Appendectomy GuidelinesДокумент12 страницAppendectomy GuidelinesJessa Frances FranciscoОценок пока нет
- Mallory Weiss SyndromeДокумент10 страницMallory Weiss SyndromeGuilherme CaneverОценок пока нет
- HerniaДокумент61 страницаHerniaAhmed HassanОценок пока нет
- Intracerebral Hemorrhage - Classification, Clinical Symptoms, DiagnosticsДокумент27 страницIntracerebral Hemorrhage - Classification, Clinical Symptoms, DiagnosticsJoisy AloorОценок пока нет
- Flail ChestДокумент5 страницFlail Chestthelazia0% (1)
- Intracerebral Hemorrhage ICHДокумент52 страницыIntracerebral Hemorrhage ICHStaporn KasemsripitakОценок пока нет
- URETEROLITHIASISДокумент21 страницаURETEROLITHIASISDhea Faizia TasyaОценок пока нет
- Final Hydrocephalus Care PlanДокумент11 страницFinal Hydrocephalus Care PlanSAYMABANUОценок пока нет
- Pneumonia treatment guide under 40 charactersДокумент1 страницаPneumonia treatment guide under 40 characters洪靖儀Оценок пока нет
- Systemic HypertensionДокумент11 страницSystemic HypertensionMeldaОценок пока нет
- AnemiaДокумент62 страницыAnemiaKay Ramos JimenoОценок пока нет
- ADPKDДокумент75 страницADPKDVenkataramanan KrishnamoorthyОценок пока нет
- Bronkiektasis: DOSEN: Dr. Merari Panti Astuti, SP - Rad Satrianti Totting (42170175)Документ43 страницыBronkiektasis: DOSEN: Dr. Merari Panti Astuti, SP - Rad Satrianti Totting (42170175)quinnОценок пока нет
- Wound Dressing JurnalДокумент32 страницыWound Dressing JurnalMuhsinAnisОценок пока нет
- Dr. Jufri Latief (Compartment Syndromes)Документ11 страницDr. Jufri Latief (Compartment Syndromes)shintaОценок пока нет
- Hernia AbdominalisДокумент45 страницHernia AbdominalisFAIRUZ RIFANIОценок пока нет
- Penyakit Jantung Iskemik: Dr. Abraham Avicenna, SPJPДокумент31 страницаPenyakit Jantung Iskemik: Dr. Abraham Avicenna, SPJPradian diptaОценок пока нет
- Acute Coronary SyndromeДокумент42 страницыAcute Coronary SyndromeGorgieОценок пока нет
- 2 - PPT DR Erika Maharani SPJPДокумент42 страницы2 - PPT DR Erika Maharani SPJPAmry YusufОценок пока нет
- Assessment Report: Clopidogrel/Acetylsalicylic Acid MylanДокумент50 страницAssessment Report: Clopidogrel/Acetylsalicylic Acid MylanDede KurniawanОценок пока нет
- Mitral Valve Prolapse (MVP) : Auscultation of MurmursДокумент55 страницMitral Valve Prolapse (MVP) : Auscultation of MurmursYagyeshОценок пока нет
- Current Trends in Cardio Vascular Nursing - PresentationДокумент42 страницыCurrent Trends in Cardio Vascular Nursing - Presentationmikegrace0289% (9)
- Aha Acls Prep Packet 2020Документ69 страницAha Acls Prep Packet 2020VP The Hacker100% (2)
- CBD 5 - NstemiДокумент11 страницCBD 5 - NstemiA MОценок пока нет
- Cobas h232 Primary Care BrochureДокумент12 страницCobas h232 Primary Care Brochurerizal_aspanОценок пока нет
- "Is There A Doctor On Board - " The Plight of The In-Flight Orthopaedic SurgeonДокумент8 страниц"Is There A Doctor On Board - " The Plight of The In-Flight Orthopaedic SurgeonRajiv TanwarОценок пока нет
- Acute Coronary SyndromesДокумент47 страницAcute Coronary SyndromeshorosuОценок пока нет
- Unstable AnginaДокумент11 страницUnstable AnginaAdrian BoboceaОценок пока нет
- Acute Coronary Syndrome - Manchester Students 23.11.2020Документ27 страницAcute Coronary Syndrome - Manchester Students 23.11.2020Dalila ZildžićОценок пока нет
- Red Cross Als Prep Packet 2022 1Документ58 страницRed Cross Als Prep Packet 2022 1Robert MccallumОценок пока нет
- Essentials of Internal MedicineДокумент832 страницыEssentials of Internal MedicineEmanuelMC100% (74)
- Acute Coronary Syndrome and Coronary Heart Disease GuideДокумент29 страницAcute Coronary Syndrome and Coronary Heart Disease GuideDwi Akbarina YahyaОценок пока нет
- A New Clinical Classification of Acute Myocardial InfarctionДокумент6 страницA New Clinical Classification of Acute Myocardial InfarctionMariaVirginiaОценок пока нет
- Clinical Spectrum of Atherosclerotic Heart DiseaseДокумент50 страницClinical Spectrum of Atherosclerotic Heart Diseaseadamu mohammadОценок пока нет
- TroponinДокумент78 страницTroponinLidya MustikasariОценок пока нет
- Prasugrel Vs Tikagrelor AppendixДокумент34 страницыPrasugrel Vs Tikagrelor AppendixSlobodan ObradovicОценок пока нет
- Unstable AnginaДокумент20 страницUnstable AnginaMoon AudioОценок пока нет
- MSLIF08 Quantitative Immunofluorescence AnalyzerДокумент2 страницыMSLIF08 Quantitative Immunofluorescence AnalyzerVictoria AnnaОценок пока нет
- Experience With A Chest Pain CenterДокумент8 страницExperience With A Chest Pain CenterGabriel Cadavid GilОценок пока нет
- Aha Acls Algorithms 2010Документ13 страницAha Acls Algorithms 2010Imania AssagafОценок пока нет
- The UP-Philippine General Hospital Acute Coronary Events at The Emergency Room Registry (UP PGH-ACER)Документ11 страницThe UP-Philippine General Hospital Acute Coronary Events at The Emergency Room Registry (UP PGH-ACER)Camille MalilayОценок пока нет
- UVA Family Medicine Qbank Answers PDFДокумент101 страницаUVA Family Medicine Qbank Answers PDFjamesmgang100% (1)
- Myocardial Infarction 2017Документ12 страницMyocardial Infarction 2017Mateo Daniel Gutierrez CastañedaОценок пока нет
- ACS Case StudyДокумент26 страницACS Case StudyMari Lyn100% (1)
- TheProtocolBookforIntensiveCare2C4eNov302C20139350907402JaypeeBrothersMedicalPub PDFДокумент540 страницTheProtocolBookforIntensiveCare2C4eNov302C20139350907402JaypeeBrothersMedicalPub PDFMaria Lisa WijayaОценок пока нет
- Ischaemic Heart Disease: DR Haider Baqai Assistant Professor of Medicine Rawalpindi Medical CollegeДокумент104 страницыIschaemic Heart Disease: DR Haider Baqai Assistant Professor of Medicine Rawalpindi Medical CollegeputriluftiОценок пока нет
- Acute Coronary Syndrome: Diagnosis and Initial Management: Each YearДокумент9 страницAcute Coronary Syndrome: Diagnosis and Initial Management: Each YearGabriela Pacheco0% (1)
- Acute Coronary Syndromes Signs SymptomsДокумент17 страницAcute Coronary Syndromes Signs Symptomssulesa askawiОценок пока нет