Вам также может понравиться
- Gen 017 - SasДокумент6 страницGen 017 - SasJames Eugene Quilinderino CaasiОценок пока нет
- GEN 017 - SAS Lesson #9Документ5 страницGEN 017 - SAS Lesson #9Faith CalimlimОценок пока нет
- Nutrition (LAB) SAS23Документ7 страницNutrition (LAB) SAS23nicoleangela ubasroselloОценок пока нет
- Spiritual care nursing lessonДокумент2 страницыSpiritual care nursing lessonFaith CalimlimОценок пока нет
- MCN 109 A Well High Risk Compilation of ExamsДокумент204 страницыMCN 109 A Well High Risk Compilation of ExamsChristine Airah TanaligaОценок пока нет
- Einc ReviewerДокумент4 страницыEinc ReviewerEricson Candelaria0% (1)
- PRELIMS 219 Q - uPDATEDДокумент8 страницPRELIMS 219 Q - uPDATEDAloha ItsmeОценок пока нет
- Nursing Care Plans for Labor Pain and AnxietyДокумент7 страницNursing Care Plans for Labor Pain and AnxietyJP2001Оценок пока нет
- Name: Age: Sex: Weight (KG) : Height/Length (CM) : Temperature (°C) : Ask: What Are The Child's Problems Initial Visit? Follow-Up Visit? DateДокумент4 страницыName: Age: Sex: Weight (KG) : Height/Length (CM) : Temperature (°C) : Ask: What Are The Child's Problems Initial Visit? Follow-Up Visit? DateCharmagne Yanga EpantoОценок пока нет
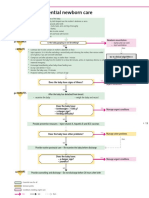
- Essential newborn care steps in first 90 minutesДокумент1 страницаEssential newborn care steps in first 90 minutesGabriel Anthony ArtizaОценок пока нет
- Drug Study FinalsДокумент4 страницыDrug Study FinalsKathleen Dela CruzОценок пока нет
- Common Side Effects of Oxytocin Include:: CNS: Maternal: COMAДокумент3 страницыCommon Side Effects of Oxytocin Include:: CNS: Maternal: COMAann camposОценок пока нет
- Mae Ann Oliva Valic - BIOETHICS SAS10Документ5 страницMae Ann Oliva Valic - BIOETHICS SAS10Mae Ann Oliva ValicОценок пока нет
- SAS Session 3 Research 1Документ5 страницSAS Session 3 Research 1Leaflor Ann ManghihilotОценок пока нет
- MS Rle Go, So, Dpa, Assessment (07-29-21)Документ8 страницMS Rle Go, So, Dpa, Assessment (07-29-21)Rhea Mala-Ay TorregosaОценок пока нет
- GEN 017: Religions, Religious Practices and Spirituality Student Activity Sheet Lesson #10Документ7 страницGEN 017: Religions, Religious Practices and Spirituality Student Activity Sheet Lesson #10Angelica Dalit MendozaОценок пока нет
- Immediate Newborn Care Definition 23Документ6 страницImmediate Newborn Care Definition 23Courtney Dela FierraОценок пока нет
- Obstetrical History and Assessment ActivityДокумент3 страницыObstetrical History and Assessment ActivityNielette R. BASALОценок пока нет
- Retig Erick Angelo Computation Aog EdcДокумент3 страницыRetig Erick Angelo Computation Aog EdcAngelo RetigОценок пока нет
- Nursing Care of a Toddler and FamilyДокумент6 страницNursing Care of a Toddler and FamilyIan Mendez100% (1)
- School of Health and Allied Health Sciences Nursing Department Self-Directed Learning (Nur 146 - Clinical Area)Документ5 страницSchool of Health and Allied Health Sciences Nursing Department Self-Directed Learning (Nur 146 - Clinical Area)Milagros FloritaОценок пока нет
- Nursing Care for Children with Immune DisordersДокумент19 страницNursing Care for Children with Immune Disordersclaire yowsОценок пока нет
- Sumbad - AOG and EDC ComputationДокумент1 страницаSumbad - AOG and EDC ComputationDredd Alejo SumbadОценок пока нет
- Pre Term Case OlieДокумент10 страницPre Term Case OlieKimsha ConcepcionОценок пока нет
- M5 Module 12G-26203Документ33 страницыM5 Module 12G-26203Ruthangela Garcia100% (1)
- Nursing Care Plan Placenta PreviaДокумент2 страницыNursing Care Plan Placenta PreviaApril Ann HortilanoОценок пока нет
- Assessment Nursing Diagnosis Goal/ Objective Intervention EvaluationДокумент1 страницаAssessment Nursing Diagnosis Goal/ Objective Intervention Evaluationjezreel ibarraОценок пока нет
- TerramycinДокумент2 страницыTerramycinChoox PriiОценок пока нет
- Care of Patient With Pregnancy Uterine Delivered by Primary Cs Secondary To Cephalopelvic DisproportionДокумент38 страницCare of Patient With Pregnancy Uterine Delivered by Primary Cs Secondary To Cephalopelvic DisproportionLuayon Francis100% (1)
- Nur 145 (Exam Gina) : Concealed HemorrhageДокумент26 страницNur 145 (Exam Gina) : Concealed HemorrhageAntoinette PeleñaОценок пока нет
- WVSU College of Nursing Drug StudyДокумент2 страницыWVSU College of Nursing Drug StudyPrisHee YhaRz SalvadorОценок пока нет
- Managing Labor Pain NaturallyДокумент2 страницыManaging Labor Pain Naturallyjay kusainОценок пока нет
- Health Promotion of The Toddler and FamilyДокумент44 страницыHealth Promotion of The Toddler and FamilyJuanaly BadiolaОценок пока нет
- Weekly Course Learning Objectives (Postpartum)Документ4 страницыWeekly Course Learning Objectives (Postpartum)Reyna Mee AhiyasОценок пока нет
- Nursing Informatics Timeline (CENIZA BSN 3E)Документ1 страницаNursing Informatics Timeline (CENIZA BSN 3E)FATIMA IVAN S. CENIZAОценок пока нет
- HES 032 BSN - Lecture Comprehensive ExamДокумент47 страницHES 032 BSN - Lecture Comprehensive ExamDIAZ, GIANNA D.Оценок пока нет
- General Objective: College of NursingДокумент3 страницыGeneral Objective: College of NursingRaan Lade KilemОценок пока нет
- Reflection 1Документ5 страницReflection 1api-400554289Оценок пока нет
- Care of New Born Basic Care of Normal NeonatesДокумент4 страницыCare of New Born Basic Care of Normal NeonatesSREEDEVI T SURESHОценок пока нет
- BSN 2A Garcia Essential Intrapartum and Newborn Care RationaleДокумент5 страницBSN 2A Garcia Essential Intrapartum and Newborn Care RationaleBellarmine MillenaОценок пока нет
- Essential Intrapartum Newborn Care: Prepared byДокумент41 страницаEssential Intrapartum Newborn Care: Prepared byJayrelle D. Safran100% (1)
- Hepatitis B vaccine mechanism of action, indications, contraindications, adverse effects and nursing responsibilitiesДокумент1 страницаHepatitis B vaccine mechanism of action, indications, contraindications, adverse effects and nursing responsibilitiesSeno HyeonОценок пока нет
- Ballard Gestational Age AssessmentДокумент8 страницBallard Gestational Age AssessmentgailОценок пока нет
- C-Section Case StudyДокумент4 страницыC-Section Case StudyChin Villanueva Ulam0% (1)
- Benefits of Breastfeeding for Mothers and BabiesДокумент25 страницBenefits of Breastfeeding for Mothers and BabiesWengel RedkissОценок пока нет
- Case 1Документ1 страницаCase 1Patricia Ysabelle LedesmaОценок пока нет
- Bag Technique 2 UCДокумент2 страницыBag Technique 2 UCSoleil Maxwell0% (1)
- First Step To Achieve Your Objective - GomezДокумент8 страницFirst Step To Achieve Your Objective - GomezNicole Ivy GorimoОценок пока нет
- PERCEPTION-COORDINATION-PRE-TEST RationalizationДокумент11 страницPERCEPTION-COORDINATION-PRE-TEST Rationalizationdrei yanОценок пока нет
- Nursing Care of Children with Respiratory IllnessesДокумент44 страницыNursing Care of Children with Respiratory IllnessesAmy Del Carmen0% (1)
- Dysfunctional Uterine Bleeding (DUB)Документ1 страницаDysfunctional Uterine Bleeding (DUB)Bheru LalОценок пока нет
- Family Nursing Care Plan1Документ2 страницыFamily Nursing Care Plan1Karlo ReyesОценок пока нет
- Abruptio Placenta NCPДокумент2 страницыAbruptio Placenta NCPjohncarlo ramos100% (1)
- PA Tool Sample - JIJIДокумент35 страницPA Tool Sample - JIJIJirah RuedasОценок пока нет
- Workplan Rle JuneДокумент18 страницWorkplan Rle JuneQueeny Anne Apil33% (3)
- Individual Activity 3 PDFДокумент11 страницIndividual Activity 3 PDFBanana QОценок пока нет
- ZegenДокумент2 страницыZegenianecunar100% (3)
- Discharge PlanДокумент3 страницыDischarge PlanDranlie LagdamenОценок пока нет
- Young InfantДокумент69 страницYoung InfantAurora Doris BatagaОценок пока нет
- Young InfantДокумент69 страницYoung InfantAurora Doris BatagaОценок пока нет
- WOMEN'S HEALTH 2019with VIDEOДокумент73 страницыWOMEN'S HEALTH 2019with VIDEOAurora Doris BatagaОценок пока нет
- WOMEN'S HEALTH 2019with VIDEOДокумент73 страницыWOMEN'S HEALTH 2019with VIDEOAurora Doris BatagaОценок пока нет
- Breastfeeding Benefits and Best PracticesДокумент49 страницBreastfeeding Benefits and Best PracticesAurora Doris BatagaОценок пока нет
- Young InfantДокумент69 страницYoung InfantAurora Doris BatagaОценок пока нет
- Young InfantДокумент69 страницYoung InfantAurora Doris BatagaОценок пока нет
- Women's Health 2019with VideoДокумент72 страницыWomen's Health 2019with VideoAurora Doris BatagaОценок пока нет
- Jaw RelationsДокумент44 страницыJaw Relationsjquin3100% (1)
- Child AbuseДокумент3 страницыChild AbuseUthuriel27Оценок пока нет
- Low Cost Ventilator With BGM and OximeterДокумент6 страницLow Cost Ventilator With BGM and OximeterVIVA-TECH IJRIОценок пока нет
- Gender Inequality & Its Impact On Mental HealthДокумент22 страницыGender Inequality & Its Impact On Mental Healthbanipreet kaurОценок пока нет
- Checklist of Documentary Requirements Maternity Benefit Reimbursement ApplicationДокумент3 страницыChecklist of Documentary Requirements Maternity Benefit Reimbursement Applicationrhianne_lhen5824Оценок пока нет
- Quality Management System: Department: Rolling Mill - Ii Section: Operation (BSM) Responsibility & AuthorityДокумент34 страницыQuality Management System: Department: Rolling Mill - Ii Section: Operation (BSM) Responsibility & AuthoritysourajpatelОценок пока нет
- Byproducts Utilization from Wheat Milling for Value Added ProductsДокумент88 страницByproducts Utilization from Wheat Milling for Value Added ProductsSivamani SelvarajuОценок пока нет
- Hamilton County Infant Mortality RatesДокумент3 страницыHamilton County Infant Mortality RatesWCPO 9 NewsОценок пока нет
- Fundamentals of Nursing: Urinary Elimination, Catheterization, Ostomy Care & Pain ManagementДокумент29 страницFundamentals of Nursing: Urinary Elimination, Catheterization, Ostomy Care & Pain ManagementKatrina Issa A. GelagaОценок пока нет
- Health declaration formДокумент1 страницаHealth declaration formGinalyn DiloyОценок пока нет
- IB Chemistry SL Revision Option DДокумент6 страницIB Chemistry SL Revision Option DMinh MinhОценок пока нет
- 2015 ESC Guidelines For The Management of Infective EndocarditisДокумент54 страницы2015 ESC Guidelines For The Management of Infective EndocarditisFernando Muñoz SolteroОценок пока нет
- ESICM EDIC Part I exam guideДокумент6 страницESICM EDIC Part I exam guideErlan SantosОценок пока нет
- Cva (Npte)Документ16 страницCva (Npte)papermannerОценок пока нет
- 187340592059Документ100 страниц187340592059Kashish PatelОценок пока нет
- Case Study On LEUKEMIAДокумент55 страницCase Study On LEUKEMIAmacky90% (21)
- Benefits of GLP Compliance in MalaysiaДокумент10 страницBenefits of GLP Compliance in MalaysiapremasarthyОценок пока нет
- Getting The Most Out of The Fit Note GP GuidanceДокумент28 страницGetting The Most Out of The Fit Note GP GuidanceLaurensia Erlina NataliaОценок пока нет
- Nelson2014 Hialuronidase em HematomasДокумент3 страницыNelson2014 Hialuronidase em HematomasPaula AzevedoОценок пока нет
- HattttДокумент15 страницHattttFrences Ann VillamorОценок пока нет
- Nijukti Khabar 21 - 27 April 2012Документ16 страницNijukti Khabar 21 - 27 April 2012pratidinОценок пока нет
- Ellen Respiratory Module PortraitДокумент11 страницEllen Respiratory Module PortraitAbdelmar SusulanОценок пока нет
- Mental Disorders StudyДокумент4 страницыMental Disorders StudyShenali NadeeshaОценок пока нет
- Ajptr 35003 3 - 7103Документ18 страницAjptr 35003 3 - 7103Naomita JoiceОценок пока нет
- ReferДокумент189 страницReferrameshОценок пока нет
- Lilongwe University Child Rights AssignmentДокумент6 страницLilongwe University Child Rights Assignmentgift ChaulukaОценок пока нет
- METABOLISM AND THERMOREGULATIONДокумент44 страницыMETABOLISM AND THERMOREGULATIONriezanurdinsyahОценок пока нет
- Spinning Mill ProcessДокумент10 страницSpinning Mill ProcessAnees PainkalОценок пока нет
- Levels of Organization Answers PDFДокумент3 страницыLevels of Organization Answers PDFKevin Ear Villanueva100% (4)
- Level 3 Health and Social Care PackДокумент735 страницLevel 3 Health and Social Care PackGeorgiana Deaconu100% (4)