Вам также может понравиться
- NICU PPT Hypo and HyperthermiaДокумент23 страницыNICU PPT Hypo and HyperthermiaelsawzgoodОценок пока нет
- HypothermiaДокумент23 страницыHypothermiaKahfi Rakhmadian KiraОценок пока нет
- Hypothermia in Neonates PresentationДокумент18 страницHypothermia in Neonates PresentationIshОценок пока нет
- Essential Newborn CareДокумент67 страницEssential Newborn CareTadesse MuhammedОценок пока нет
- Essential Newborn Care: Dr. Sumitra Kumara Meena Senior Resident, Pediatrics Safdarjung Hospital, New DelhiДокумент75 страницEssential Newborn Care: Dr. Sumitra Kumara Meena Senior Resident, Pediatrics Safdarjung Hospital, New DelhiDr Divyarani D CОценок пока нет
- Minor Ailments of Newborn NewДокумент47 страницMinor Ailments of Newborn NewPOORNIMA B SОценок пока нет
- PREMATURITYДокумент40 страницPREMATURITYBlykeBantuganОценок пока нет
- Therapeutic PlayДокумент9 страницTherapeutic PlayVivek PrabhakarОценок пока нет
- Nursing Care For NewbornДокумент33 страницыNursing Care For NewbornDarla Quiballo100% (1)
- Recommended Standards For Newborn ICU DesignДокумент18 страницRecommended Standards For Newborn ICU DesignYayang Andayani100% (1)
- Newborn CareДокумент49 страницNewborn CareJohn Mark PocsidioОценок пока нет
- High Risk New BornДокумент12 страницHigh Risk New BornM. jehovah Nissie YeshalomeОценок пока нет
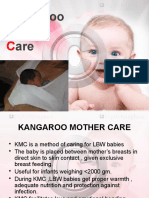
- Standard Operating Procedures For Kangaroo Mother CareДокумент2 страницыStandard Operating Procedures For Kangaroo Mother Caremarisa_ichsanОценок пока нет
- Breast FeedingДокумент3 страницыBreast FeedingArla Donissa-Donique Castillon AlviorОценок пока нет
- Minordisordersofbnewborn 161129154708Документ33 страницыMinordisordersofbnewborn 161129154708Kevin Daniel GoveasОценок пока нет
- Paediatrics - Febrile Convulsions Assessment, Treatment and Education PDFДокумент12 страницPaediatrics - Febrile Convulsions Assessment, Treatment and Education PDFPalash NagdeoteОценок пока нет
- Care of Child in IncubatorДокумент12 страницCare of Child in IncubatorSundaraBharathiОценок пока нет
- 03.chronic Supp Otitis MediaДокумент33 страницы03.chronic Supp Otitis MediaJumanne JayОценок пока нет
- Hypertrophic Pyloric StenosisДокумент23 страницыHypertrophic Pyloric StenosisRahel Imelda PanggabeanОценок пока нет
- Birth InjuriesДокумент11 страницBirth Injuriesdapurna86Оценок пока нет
- NewbornДокумент45 страницNewbornkiran kumarОценок пока нет
- Amniotic Fluid & Its AbnormalitiesДокумент29 страницAmniotic Fluid & Its AbnormalitiesSTAR Plus SerialsОценок пока нет
- CHAPTER 3-LactationДокумент12 страницCHAPTER 3-LactationMaria Alexis Ahadain OlvidoОценок пока нет
- Incubator CareДокумент11 страницIncubator Caremohammedruby100% (3)
- Introduction To Pediatric NursingДокумент36 страницIntroduction To Pediatric Nursingcharan poonia100% (1)
- Case Report "Febrile Seizures": Betsheba E. S. 123307018Документ37 страницCase Report "Febrile Seizures": Betsheba E. S. 123307018AmandaRizkaОценок пока нет
- Assessment and Management of High Risk Neonates DrLawHN PDFДокумент45 страницAssessment and Management of High Risk Neonates DrLawHN PDFShiva KarthikeyanОценок пока нет
- Maternal and Child Health CareДокумент12 страницMaternal and Child Health CarePraachii SharmaОценок пока нет
- Kangaroo Mother CareДокумент21 страницаKangaroo Mother CareM Fathur Arief KurniawanОценок пока нет
- Newborn CareДокумент30 страницNewborn CareAlexandria P. OrcajadaОценок пока нет
- Neonatal JaundiceДокумент36 страницNeonatal JaundiceJenaffer Achamma JohnОценок пока нет
- Neonatal Seizures and Management: Dhaka Sishu Hospital BangladeshДокумент19 страницNeonatal Seizures and Management: Dhaka Sishu Hospital BangladeshGoha BashaОценок пока нет
- Nursing Care of A Neonate Part 1Документ67 страницNursing Care of A Neonate Part 1Rani G SОценок пока нет
- Differentiate Between With AnswersДокумент14 страницDifferentiate Between With AnswersStephy SojanОценок пока нет
- Topic - Preventive Pediatrics Subject - Pediatrics Unit - IiДокумент10 страницTopic - Preventive Pediatrics Subject - Pediatrics Unit - IiDinesh KhinchiОценок пока нет
- FamilyДокумент19 страницFamilyVaishnavee Singh100% (1)
- P PyrexiaДокумент23 страницыP PyrexiaRex BishopОценок пока нет
- Nursing Care of at Risk/ High Risk/ Sick ClientДокумент256 страницNursing Care of at Risk/ High Risk/ Sick ClientAaron ConstantinoОценок пока нет
- Feeding of High Risk Neonates: Feeding of LBW Infants: How Is It Different?Документ22 страницыFeeding of High Risk Neonates: Feeding of LBW Infants: How Is It Different?sandeepv08Оценок пока нет
- HYPERBILIRUBINEMIAДокумент30 страницHYPERBILIRUBINEMIAAlexisRoyE100% (1)
- New Born Care: Catheter SuctioningДокумент17 страницNew Born Care: Catheter SuctioningRaffy100% (1)
- Newborn Assessment by DR Dahir123Документ84 страницыNewborn Assessment by DR Dahir123Najjuma BettyОценок пока нет
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesОт EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesОценок пока нет
- Name: Iniovorua Ajokperoghene: - GROUP: IM-450 - Date: 7 NOVEMBER, 2020. - Theme: DracunculiasisДокумент10 страницName: Iniovorua Ajokperoghene: - GROUP: IM-450 - Date: 7 NOVEMBER, 2020. - Theme: DracunculiasisValentina IniovoruaОценок пока нет
- WelcomeДокумент103 страницыWelcomeLyka BernalОценок пока нет
- Ten Steps To Breast Feeding and Fetal CirculationДокумент42 страницыTen Steps To Breast Feeding and Fetal CirculationKwin IbaliОценок пока нет
- Extremely Low Birth Weight (ELBW) InfantДокумент48 страницExtremely Low Birth Weight (ELBW) InfanthannanyusofОценок пока нет
- Notes On Baby Bath - Care of The Mother During The Postpartum PeriodДокумент12 страницNotes On Baby Bath - Care of The Mother During The Postpartum PeriodOink TopusОценок пока нет
- Pyloric StenosisДокумент2 страницыPyloric Stenosisgeorgeloto12Оценок пока нет
- Hyperbilirubinemia Teaching PlanДокумент2 страницыHyperbilirubinemia Teaching Planapi-25291041167% (3)
- Febrile Convulsions in ChildrenДокумент2 страницыFebrile Convulsions in ChildrenMagdalena Dwiyani HutajuluОценок пока нет
- Exercises To Facilitate Change of Baby's Position From Breech To CephalicДокумент3 страницыExercises To Facilitate Change of Baby's Position From Breech To CephalicaziskarnОценок пока нет
- Infant Radiant WarmerДокумент7 страницInfant Radiant WarmerManish MandaviyaОценок пока нет
- National Control of Dirrheal Diseases (CDD) Program ObjectivesДокумент6 страницNational Control of Dirrheal Diseases (CDD) Program ObjectivesJoy FucananОценок пока нет
- Harika Priyanka. K Asst. Professor AconДокумент30 страницHarika Priyanka. K Asst. Professor AconArchana MoreyОценок пока нет
- Postnatal CareДокумент34 страницыPostnatal CareApin PokhrelОценок пока нет
- Altered Body Temperature: Submitted To: Mrs - Ipsita Sahoo Submitted By: Krushna Priya Nayak Msc. Nursing (First Year)Документ43 страницыAltered Body Temperature: Submitted To: Mrs - Ipsita Sahoo Submitted By: Krushna Priya Nayak Msc. Nursing (First Year)Sandeep MohanОценок пока нет
- Management of Breast FeedingДокумент17 страницManagement of Breast FeedingUday KumarОценок пока нет
- 56 Ambiguous GenitaliaДокумент8 страниц56 Ambiguous GenitalianasibdinОценок пока нет
- Fanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandFanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Advt No 17 2021 Engl 261121Документ18 страницAdvt No 17 2021 Engl 261121RajaОценок пока нет
- Guru Gobind Singh Medical College & Hospital, FaridkotДокумент6 страницGuru Gobind Singh Medical College & Hospital, FaridkotRajaОценок пока нет
- Detailed Advt Teaching Position With Application FormДокумент19 страницDetailed Advt Teaching Position With Application FormRajaОценок пока нет
- Gynecological and Obstetrics InstrumentsДокумент61 страницаGynecological and Obstetrics InstrumentsRaja33% (3)
- Lesson Plan: Subject: Sociology Topic: Social ControlДокумент29 страницLesson Plan: Subject: Sociology Topic: Social ControlRaja100% (5)
- Congenital Heart DiseaseДокумент13 страницCongenital Heart DiseaseRaja86% (7)
- Obg Qus Set 3Документ24 страницыObg Qus Set 3RajaОценок пока нет
- Course & Unit Plan OBG III BSCДокумент11 страницCourse & Unit Plan OBG III BSCRaja100% (4)
- Lesson Plan On Abortions: Submitted By-Ms Sneha Sehrawat TutorДокумент21 страницаLesson Plan On Abortions: Submitted By-Ms Sneha Sehrawat TutorRaja100% (4)
- Check List of Skill Stations For Osce/Ospe Examination System of Anm® CourseДокумент36 страницCheck List of Skill Stations For Osce/Ospe Examination System of Anm® CourseRajaОценок пока нет
- Displacement of The UterusДокумент32 страницыDisplacement of The UterusRaja100% (1)
- SMS Batch 2013 PDFДокумент13 страницSMS Batch 2013 PDFRajaОценок пока нет
- Lesson Plan On Abortions: Submitted By-Ms Sneha Sehrawat TutorДокумент21 страницаLesson Plan On Abortions: Submitted By-Ms Sneha Sehrawat TutorRaja100% (4)
- Biographic DataДокумент30 страницBiographic DataRaja100% (1)
- New Microsoft Word DocumentДокумент1 страницаNew Microsoft Word DocumentRajaОценок пока нет
- The State of Uttarakhand Is Bordering Himachal Pradesh in The North-West and UttarДокумент5 страницThe State of Uttarakhand Is Bordering Himachal Pradesh in The North-West and UttarRajaОценок пока нет
- Clinical Requirements Time Schedule III OBGДокумент4 страницыClinical Requirements Time Schedule III OBGRajaОценок пока нет
- Benign Tumor Malignant Tumor: Ms. Sneha Sehrawat AIIMS RishikeshДокумент37 страницBenign Tumor Malignant Tumor: Ms. Sneha Sehrawat AIIMS RishikeshRajaОценок пока нет
- Unit Allotment OBG 3rd BSCДокумент1 страницаUnit Allotment OBG 3rd BSCRajaОценок пока нет
- College of Nursing All India Instutite of Medical Sciences, Rishikesh (Uttarakhand) B.Sc. (Hons) Nursing 3 Year Batch - 2016 End Term Examination - 2019 Subject - Maternal Health NursingДокумент24 страницыCollege of Nursing All India Instutite of Medical Sciences, Rishikesh (Uttarakhand) B.Sc. (Hons) Nursing 3 Year Batch - 2016 End Term Examination - 2019 Subject - Maternal Health NursingRajaОценок пока нет
- Urine Specimen Collection: Ms. Sneha SehrawatДокумент36 страницUrine Specimen Collection: Ms. Sneha SehrawatRajaОценок пока нет
- How To Fill The Online Form PHDДокумент5 страницHow To Fill The Online Form PHDRajaОценок пока нет
- Infant of Diabetic MotherДокумент68 страницInfant of Diabetic MotherRaja100% (5)
- Pre-Prof Final Question PaperДокумент56 страницPre-Prof Final Question PaperRajaОценок пока нет
- Patrick Duff, M.D. University of FloridaДокумент57 страницPatrick Duff, M.D. University of FloridaRajaОценок пока нет
- HIV in PregnancyДокумент28 страницHIV in PregnancyRaja100% (1)
- VF (Kyhkkjrh VK Qfozkkulalfkku) - F'KDS"K) MRRJK (K.M& 249201Документ3 страницыVF (Kyhkkjrh VK Qfozkkulalfkku) - F'KDS"K) MRRJK (K.M& 249201RajaОценок пока нет
- Urine Specimen Collection: Ms. Sneha SehrawatДокумент36 страницUrine Specimen Collection: Ms. Sneha SehrawatRajaОценок пока нет
- Hemolytic Disease of NewbornДокумент41 страницаHemolytic Disease of NewbornRaja100% (3)
- CTTДокумент47 страницCTTleizelgalvezОценок пока нет
- Daftar PustakaДокумент3 страницыDaftar PustakaEKAОценок пока нет
- Persuasive Essay - Final DraftДокумент10 страницPersuasive Essay - Final DraftEmily LongОценок пока нет
- Detecting The Differences Radiculopathy, Myelopathy and Peripheral NeuropathyДокумент70 страницDetecting The Differences Radiculopathy, Myelopathy and Peripheral Neuropathyapi-19502000100% (8)
- Myths of DialysisДокумент26 страницMyths of DialysisSijo Muthukad M100% (1)
- Extraoral Periapical Radiography An Alternative Approach To Intraoral Periapical RadiographyДокумент5 страницExtraoral Periapical Radiography An Alternative Approach To Intraoral Periapical RadiographysevattapillaiОценок пока нет
- Hydra FacialДокумент34 страницыHydra FacialDrAmit Gaba MdsОценок пока нет
- Mental Health Act Ten LawДокумент8 страницMental Health Act Ten LawAbigail BrillantesОценок пока нет
- Occupational Health NursingДокумент22 страницыOccupational Health NursingIrene Joy ArellanoОценок пока нет
- Storgard Channing WP2Документ6 страницStorgard Channing WP2Channing StorgardОценок пока нет
- Varicose VeinДокумент22 страницыVaricose VeinKamalОценок пока нет
- Quarter 1 SUMMATIVE TEST For Beauty CareДокумент4 страницыQuarter 1 SUMMATIVE TEST For Beauty CareVinzMontederamosMalupa-Jimenez100% (2)
- Chronic Renal FailureДокумент18 страницChronic Renal FailureJoan Carla BocoОценок пока нет
- Olympian Benchmark - 400mДокумент15 страницOlympian Benchmark - 400merwandumontОценок пока нет
- 2023 Vein AnatomyДокумент6 страниц2023 Vein AnatomyKarenОценок пока нет
- CRITICAL THINKING CASE STUDY - PharmaДокумент4 страницыCRITICAL THINKING CASE STUDY - PharmaElleОценок пока нет
- Glucose-Loesung 5 08-07 03Документ2 страницыGlucose-Loesung 5 08-07 03Andreea CaticiОценок пока нет
- Article1380371399 - Okigbo Et AlДокумент10 страницArticle1380371399 - Okigbo Et AlDiannokaIhzaGanungОценок пока нет
- Aplastic AnemiaДокумент3 страницыAplastic AnemiaFrancis JuneОценок пока нет
- Hypoxic Ischemic Hypoxic Ischemic E HL H E HL H Encephalopathty EncephalopathtyДокумент34 страницыHypoxic Ischemic Hypoxic Ischemic E HL H E HL H Encephalopathty EncephalopathtyKatrinaTandoc100% (1)
- SyllabusДокумент4 страницыSyllabusMădă IorgaОценок пока нет
- Comp ReДокумент15 страницComp ReROBERT C. REÑA, BSN, RN, MAN (ue)Оценок пока нет
- The Longmire I, II, and III Operations: L. William Traverso, M.D.Документ8 страницThe Longmire I, II, and III Operations: L. William Traverso, M.D.Abu ZidaneОценок пока нет
- Investigation of The Phenomenon of Propagated Sensation Along The Channels in The Upper Limb Following Administration of Acupuncture and Mock LaserДокумент10 страницInvestigation of The Phenomenon of Propagated Sensation Along The Channels in The Upper Limb Following Administration of Acupuncture and Mock LaserSebastiano SerraОценок пока нет
- PSYCHE Mental Health Concepts N2018 Ans KeyДокумент5 страницPSYCHE Mental Health Concepts N2018 Ans KeyJo Hn Vengz100% (1)
- NURSING CARE PLAN OcdДокумент25 страницNURSING CARE PLAN Ocdkiran mahal81% (26)
- PDF Document PDFДокумент8 страницPDF Document PDFDhruv AgrawalОценок пока нет
- (The Norton Library) Karen Horney - Feminine Psychology (1973, W W Norton & Co.)Документ276 страниц(The Norton Library) Karen Horney - Feminine Psychology (1973, W W Norton & Co.)daniela86% (7)
- Serotonin SyndromeДокумент19 страницSerotonin SyndromeNur Atiqah Mohd AzliОценок пока нет
- Biochemistry LaboratoryДокумент6 страницBiochemistry LaboratoryMark Benedict MontalboОценок пока нет