Вам также может понравиться
- Bujinkan Shinden Fudo Ryu Jutaijutsu DenshoДокумент6 страницBujinkan Shinden Fudo Ryu Jutaijutsu Denshomoon100% (1)
- Diabetic Foot Ulcer - Yandriyane Stephanie Robiady - 131621190504Документ28 страницDiabetic Foot Ulcer - Yandriyane Stephanie Robiady - 131621190504Yohelio Priawan SibuОценок пока нет
- Juvenile Rheumatoid ArthritisДокумент30 страницJuvenile Rheumatoid Arthritispragna VanapalaОценок пока нет
- 2002 Philadelphia Eagles Special Teams Clinic - John Harbaugh - 15 PagesДокумент15 страниц2002 Philadelphia Eagles Special Teams Clinic - John Harbaugh - 15 PagesPaul Fargo100% (1)
- 6.2 Sample Risk Assessment 2Документ3 страницы6.2 Sample Risk Assessment 2Luwalhati TomilasОценок пока нет
- Managemen Kaki Diabetika Edit DesДокумент44 страницыManagemen Kaki Diabetika Edit DesAsmawatiОценок пока нет
- Diabetic Foot Ulcer: By: FauzanadliДокумент43 страницыDiabetic Foot Ulcer: By: FauzanadliWan RahimahОценок пока нет
- Osteoarthritis (Oa) : Prakash Thakulla InternДокумент48 страницOsteoarthritis (Oa) : Prakash Thakulla InternPrakash ThakullaОценок пока нет
- Septic ArthritisДокумент38 страницSeptic ArthritisayeshasadiqamukhtarОценок пока нет
- Diabetic Foot UlcerДокумент44 страницыDiabetic Foot UlcerCandy Lee100% (1)
- Diabetic FootДокумент5 страницDiabetic FootAzi Mohamed AminОценок пока нет
- Diabetic Foot History AND ExaminationДокумент46 страницDiabetic Foot History AND ExaminationRiaОценок пока нет
- The Diabetic Foot: (Physician'S Overview)Документ43 страницыThe Diabetic Foot: (Physician'S Overview)Imtiaz AhmedОценок пока нет
- RheumatoidДокумент35 страницRheumatoidDeva LekshmiОценок пока нет
- JointsДокумент68 страницJointsLaine ZeeОценок пока нет
- Bones and Joints: Bone Is A Specialised Connective Tissue Which HasДокумент34 страницыBones and Joints: Bone Is A Specialised Connective Tissue Which HasvaishnaviОценок пока нет
- Diabetic FoootДокумент34 страницыDiabetic Foootsiakonihmat433Оценок пока нет
- Diabetic Foot Ulcer: DR Surein PrasadДокумент43 страницыDiabetic Foot Ulcer: DR Surein PrasadNinaОценок пока нет
- 6 Diabetic FootДокумент28 страниц6 Diabetic FootPraneetha NouduriОценок пока нет
- Management of Diabetic Foot Ulcers: Pandji MulyonoДокумент51 страницаManagement of Diabetic Foot Ulcers: Pandji MulyonoJeffrey Dyer100% (1)
- Diabeticfootulcer Surgicalwounds 190908030737Документ22 страницыDiabeticfootulcer Surgicalwounds 190908030737Jeevan VelanОценок пока нет
- Kaki DiabetikДокумент82 страницыKaki DiabetikNanda ValeriadiОценок пока нет
- OsteoarthritisДокумент25 страницOsteoarthritisRaymund Christopher Dela PeñaОценок пока нет
- Topic Confernce: Int Nontapat PaesarochДокумент19 страницTopic Confernce: Int Nontapat Paesarochnontapat paesarochОценок пока нет
- Diabetic Foot: Done by Saed JarrarДокумент98 страницDiabetic Foot: Done by Saed JarrarRashed ShatnawiОценок пока нет
- Rheumatoid ArthritisДокумент30 страницRheumatoid ArthritisMelisaОценок пока нет
- The Diabetic Foot: by Dr. Myrna Rita, SPRM Instalasi Rehabilitasi Medik Rsud A.W.Sjahranie, SamarindaДокумент16 страницThe Diabetic Foot: by Dr. Myrna Rita, SPRM Instalasi Rehabilitasi Medik Rsud A.W.Sjahranie, SamarindaDessy Vinoricka AndriyanaОценок пока нет
- Diabetic Foot: How Do The Pathophysiological Features of Diabetes Put The Foot at Increased Risk For Tissue Damage?Документ8 страницDiabetic Foot: How Do The Pathophysiological Features of Diabetes Put The Foot at Increased Risk For Tissue Damage?Kat BausaОценок пока нет
- Rheumatoid ArthritisДокумент52 страницыRheumatoid ArthritisArun NingarajappaОценок пока нет
- Bone andДокумент33 страницыBone andSuci MayveraОценок пока нет
- Diabetic Foot UlcerДокумент33 страницыDiabetic Foot UlceragieajОценок пока нет
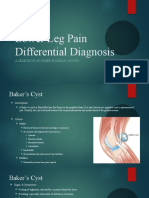
- Lower Leg Pain Differential Diagnosis - OtherДокумент13 страницLower Leg Pain Differential Diagnosis - Otherapi-619359087Оценок пока нет
- Diabetic FootДокумент73 страницыDiabetic Footmohammad.irfanОценок пока нет
- Diabetic Foot Infection: UHN AIMGP SeminarДокумент44 страницыDiabetic Foot Infection: UHN AIMGP SeminarmittulcpatelОценок пока нет
- Pencegahan & Tatalaksana Ulkus DiabetikumДокумент60 страницPencegahan & Tatalaksana Ulkus DiabetikumirhamОценок пока нет
- Diabetic FootДокумент37 страницDiabetic FootSeleno GlauberОценок пока нет
- Non Neoplastic Diseases of BoneДокумент45 страницNon Neoplastic Diseases of BoneKОценок пока нет
- 5.12 Venous UlcersДокумент4 страницы5.12 Venous UlcersCollen LihakaОценок пока нет
- باطنة تمريض rheumatologyДокумент6 страницباطنة تمريض rheumatologyAbdullmlik AlfurasОценок пока нет
- Cutaneous Manifestations of Systemic DiseasesДокумент50 страницCutaneous Manifestations of Systemic DiseasesAlex XanderОценок пока нет
- Ulcers, The Diabetic FootДокумент10 страницUlcers, The Diabetic FootmuhammadridhwanОценок пока нет
- Diabetic Foot, Diabetic Foot Ulcer & Diabetic Foot Care: Prepared by Munirah Supervised by DR NaqibДокумент49 страницDiabetic Foot, Diabetic Foot Ulcer & Diabetic Foot Care: Prepared by Munirah Supervised by DR NaqibAfifah SelamatОценок пока нет
- Diabetic FootДокумент22 страницыDiabetic FootNaikko80100% (2)
- Chronic Venous InsufficiencyДокумент4 страницыChronic Venous Insufficiencyfandi_cah_ganteng3367100% (1)
- Diabetic Foot: Sabrina Faning Yuliani Widya MarwahДокумент40 страницDiabetic Foot: Sabrina Faning Yuliani Widya Marwahaulia areta rahmaОценок пока нет
- Arthritis 180325095830 PDFДокумент77 страницArthritis 180325095830 PDFHesoca HuxОценок пока нет
- Colegenoze EnglezaДокумент47 страницColegenoze EnglezaNedelcu MirunaОценок пока нет
- Diabetic FootДокумент6 страницDiabetic FootproudofskyОценок пока нет
- IPT 12 Venous UlcersДокумент41 страницаIPT 12 Venous UlcersLAL DIME 1Оценок пока нет
- FIX Leg UlcerДокумент59 страницFIX Leg UlcerDekka Andra100% (2)
- 06 Skin Care, Aseptic Technique and Prevention For The Pressure UlcersДокумент7 страниц06 Skin Care, Aseptic Technique and Prevention For The Pressure Ulcers楊畯凱Оценок пока нет
- Faculty of MedicineДокумент28 страницFaculty of MedicineRana AtefОценок пока нет
- 6.dabetic FootДокумент81 страница6.dabetic FootArleen MatincaОценок пока нет
- Notes On AmputationsДокумент3 страницыNotes On AmputationsShaileeОценок пока нет
- Case Presentation - Diabetic FootДокумент41 страницаCase Presentation - Diabetic FootBharathbushan V MandiriОценок пока нет
- OsteomyelitisДокумент147 страницOsteomyelitisAnkit Agur100% (1)
- Chapter 14: The ArthropathiesДокумент18 страницChapter 14: The ArthropathiespoddataОценок пока нет
- Physical Therapy PerspectiveДокумент33 страницыPhysical Therapy PerspectiveRuth EstebanОценок пока нет
- Peripheral Vascular Disease and Its Physiotherapy ManagementДокумент61 страницаPeripheral Vascular Disease and Its Physiotherapy ManagementSuman DeyОценок пока нет
- Arthritis 2Документ22 страницыArthritis 2bellayuandaОценок пока нет
- Diabetic Foot + GangreneДокумент26 страницDiabetic Foot + Gangreneili_izyan100% (1)
- Bengkel Safe MotherhoodДокумент12 страницBengkel Safe MotherhoodMujahid Zurich Takaful Johor-GanuОценок пока нет
- Word Search ActivityДокумент2 страницыWord Search ActivityMujahid Zurich Takaful Johor-GanuОценок пока нет
- Hairi Celebrates Hari Raya: Worksheet Beautiful MalaysiaДокумент1 страницаHairi Celebrates Hari Raya: Worksheet Beautiful MalaysiaMujahid Zurich Takaful Johor-GanuОценок пока нет
- And or SntncesДокумент5 страницAnd or SntncesMujahid Zurich Takaful Johor-GanuОценок пока нет
- Active Passive InsufficiencyДокумент20 страницActive Passive InsufficiencyBhargav67% (6)
- Principles of Wound HealingДокумент8 страницPrinciples of Wound HealingTracy100% (6)
- Overuse Injuries and Burnout in Youth Sports A PosДокумент17 страницOveruse Injuries and Burnout in Youth Sports A PosChi Chung CHANОценок пока нет
- Radial Neck Fractures in ChildrenДокумент4 страницыRadial Neck Fractures in ChildrenAndikaОценок пока нет
- GURPS 4e - Hit Locations V3Документ9 страницGURPS 4e - Hit Locations V3Luca LiperiОценок пока нет
- Acute Respiratory Failure For StudentДокумент41 страницаAcute Respiratory Failure For Studentapi-379952350% (4)
- Emergency Radiology - Dr. YantoДокумент93 страницыEmergency Radiology - Dr. YantoLeonardus William KuswaraОценок пока нет
- Orthopedic ConditionsДокумент11 страницOrthopedic ConditionsErin Hoffmann100% (3)
- Quatrains of Nostradamus - Century VIII PDFДокумент11 страницQuatrains of Nostradamus - Century VIII PDFNishant PrabhakarОценок пока нет
- Development of Muscular System AtfДокумент3 страницыDevelopment of Muscular System AtfKim Sa-buОценок пока нет
- CRIMINOLOGY 3 - Module 4 (Barbarona)Документ28 страницCRIMINOLOGY 3 - Module 4 (Barbarona)Joe Bert ButligОценок пока нет
- Head Gestured Automated Wheelchair: Bachelor of Technology Department of MECHANICAL EngineeringДокумент42 страницыHead Gestured Automated Wheelchair: Bachelor of Technology Department of MECHANICAL EngineeringNimitesh SinghОценок пока нет
- Ratio - Neuro (VR 2.O)Документ24 страницыRatio - Neuro (VR 2.O)Accey RamirezОценок пока нет
- The Workmen Compensation ActДокумент5 страницThe Workmen Compensation Actpriyanka sharmaОценок пока нет
- 2010 05 27 Shibaricon Max Fundamentals PDFДокумент13 страниц2010 05 27 Shibaricon Max Fundamentals PDFyeltseinОценок пока нет
- Specimen/Sample Textual Questions and Answers From The Rogue' - Atulananda GoswamiДокумент2 страницыSpecimen/Sample Textual Questions and Answers From The Rogue' - Atulananda GoswamiRenan Sardar100% (1)
- MySims - Manual - WIIДокумент6 страницMySims - Manual - WIIasdasdОценок пока нет
- Grafting: Grafting and Budding Nursery Crop Plants AG-396Документ9 страницGrafting: Grafting and Budding Nursery Crop Plants AG-396Marlin GooseОценок пока нет
- Ebook Atlas of Interventional Orthopedics Procedures Essential Guide For Fluoroscopy and Ultrasound Guided Procedures PDF Full Chapter PDFДокумент68 страницEbook Atlas of Interventional Orthopedics Procedures Essential Guide For Fluoroscopy and Ultrasound Guided Procedures PDF Full Chapter PDFcharles.schmidt276100% (26)
- Knee Exam - OSCE Stations PDFДокумент2 страницыKnee Exam - OSCE Stations PDFEmiel AwadОценок пока нет
- IJCD 2017 Know Your Instrument GuideДокумент106 страницIJCD 2017 Know Your Instrument GuideYarina Nathaly Pilco RomanОценок пока нет
- ZF Repair Manaul Tranmission HBF 15 - 18-II and - 5Документ47 страницZF Repair Manaul Tranmission HBF 15 - 18-II and - 5ahmed_eng_1500100% (2)
- 23 2012 Official Signals NLFДокумент6 страниц23 2012 Official Signals NLFEthan KairosОценок пока нет
- I x27 M The Alpha x27 S MateДокумент105 страницI x27 M The Alpha x27 S MateLaurice Melepyano100% (1)
- Hirarc FormДокумент3 страницыHirarc FormSalsabilla Putri anggraini100% (1)
- Right Inguinal Hernia RepairДокумент1 страницаRight Inguinal Hernia Repairsgod34Оценок пока нет
- Hiking Jebel Hafeet ReflectionДокумент4 страницыHiking Jebel Hafeet Reflectionapi-297410574Оценок пока нет