Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- K 46 Compact Spinning Machine Brochure 2530-V3 75220 Original English 75220Документ28 страницK 46 Compact Spinning Machine Brochure 2530-V3 75220 Original English 75220Pradeep JainОценок пока нет
- (Dr. Mariam) NT40103 AssignmentДокумент11 страниц(Dr. Mariam) NT40103 AssignmentAhmad Syamil Muhamad ZinОценок пока нет
- Art of Data ScienceДокумент159 страницArt of Data Sciencepratikshr192% (12)
- Compare and Contrast Two Cultures Celebrate Between Bali and JavaДокумент1 страницаCompare and Contrast Two Cultures Celebrate Between Bali and JavaqonitazmiОценок пока нет
- Young Entrepreneurs of IndiaДокумент13 страницYoung Entrepreneurs of Indiamohit_jain_90Оценок пока нет
- Chapter 1Документ16 страницChapter 1MulugetaОценок пока нет
- Jataka Tales - The Crane and The CrabДокумент5 страницJataka Tales - The Crane and The Crabshahrajan2k1Оценок пока нет
- Lesson Plan in Explicirt Teaching in Oral Lnguage and Grammar (Checked)Документ3 страницыLesson Plan in Explicirt Teaching in Oral Lnguage and Grammar (Checked)Lovella GacaОценок пока нет
- How To Write An Argumented EssayДокумент35 страницHow To Write An Argumented EssayFarhad UllahОценок пока нет
- Young Learners Starters Sample Papers 2018 Vol1Документ15 страницYoung Learners Starters Sample Papers 2018 Vol1Natalia García GarcíaОценок пока нет
- List of Festivals in India - WikipediaДокумент13 страницList of Festivals in India - WikipediaRashmi RaviОценок пока нет
- Presentation of Times of India Newspaper SIPДокумент38 страницPresentation of Times of India Newspaper SIPPrakruti ThakkarОценок пока нет
- Nutrition and Diet Therapy ExaminationДокумент8 страницNutrition and Diet Therapy ExaminationIrwan M. Iskober100% (3)
- Julien Freund - A TributeДокумент10 страницJulien Freund - A TributeJuan Pablo SerraОценок пока нет
- Ingles Nivel 2Документ119 страницIngles Nivel 2Perla Cortes100% (1)
- Rincian Kewenangan Klinis AnakДокумент6 страницRincian Kewenangan Klinis AnakUchiha ItachiОценок пока нет
- Introduction To Biostatistics KMPK 2023Документ46 страницIntroduction To Biostatistics KMPK 2023ciciОценок пока нет
- MMW CH4 L2Документ20 страницMMW CH4 L2Charles Patrick GarciaОценок пока нет
- He Didnt Die in Vain - Take No GloryДокумент2 страницыHe Didnt Die in Vain - Take No GloryDagaerag Law OfficeОценок пока нет
- Salija, K. (2017) OutlineДокумент9 страницSalija, K. (2017) OutlineNurina UlfaОценок пока нет
- Bragg Waveguide and Its DescriptionДокумент22 страницыBragg Waveguide and Its DescriptionPratibha Karki RawatОценок пока нет
- English Preparation Guide DAF 202306Документ12 страницEnglish Preparation Guide DAF 202306TIexamesОценок пока нет
- scn615 Classroomgroupactionplan SarahltДокумент3 страницыscn615 Classroomgroupactionplan Sarahltapi-644817377Оценок пока нет
- Appendix I Leadership Questionnaire: Ior Description Questionnaire (LBDQ - Form XII 1962) - The Division IntoДокумент24 страницыAppendix I Leadership Questionnaire: Ior Description Questionnaire (LBDQ - Form XII 1962) - The Division IntoJoan GonzalesОценок пока нет
- Parallels of Stoicism and KalamДокумент95 страницParallels of Stoicism and KalamLDaggersonОценок пока нет
- Reaction On The 83RD Post Graduate Course On Occupational Health and SafetyДокумент1 страницаReaction On The 83RD Post Graduate Course On Occupational Health and SafetyEdcelle SabanalОценок пока нет
- D78846GC20 sg2Документ356 страницD78846GC20 sg2hilordОценок пока нет
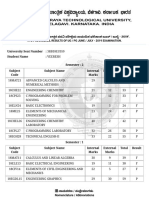
- VTU Result PDFДокумент2 страницыVTU Result PDFVaibhavОценок пока нет
- RI Prelims GP H1 Paper 2 Ans KeyДокумент18 страницRI Prelims GP H1 Paper 2 Ans Keyjaylynn6100% (1)
- 2009-Journal of Pharmacy and PharmacologyДокумент37 страниц2009-Journal of Pharmacy and PharmacologyLeticia Bonancio CerqueiraОценок пока нет