Вам также может понравиться
- Musculoskeletal Infections: Wassim Ballan, MD Pediatric Infectious DiseasesДокумент33 страницыMusculoskeletal Infections: Wassim Ballan, MD Pediatric Infectious DiseasesGufron MustofaОценок пока нет
- Surgery Case AppendicitisДокумент30 страницSurgery Case AppendicitisSarahОценок пока нет
- Fournier GanggrenДокумент13 страницFournier GanggrenAnonymous P5FDn81yОценок пока нет
- Laporan Kasus - HemorrhoidsДокумент41 страницаLaporan Kasus - HemorrhoidsMetyana CahyaningtyasОценок пока нет
- Sum 41 Inspired PerДокумент54 страницыSum 41 Inspired PerMuhammad Ihsan AuliaОценок пока нет
- Morning Report: Disusun Oleh: Noermawati DewiДокумент37 страницMorning Report: Disusun Oleh: Noermawati DewidevyОценок пока нет
- Thyroid Nodule Management and EvaluationДокумент137 страницThyroid Nodule Management and EvaluationLeiОценок пока нет
- Grandrounds Protocol ServandoДокумент4 страницыGrandrounds Protocol ServandoAllison Eunice ServandoОценок пока нет
- Oropharynx Diffuse Large B Cell Lymphoma Stadium II B (E), in 31 Weeks Multigravida PregnancyДокумент33 страницыOropharynx Diffuse Large B Cell Lymphoma Stadium II B (E), in 31 Weeks Multigravida PregnancyYosua SugiantoОценок пока нет
- Morning Report: Patient with Seizure and FeverДокумент34 страницыMorning Report: Patient with Seizure and FeverdevyОценок пока нет
- Choledochal CystДокумент68 страницCholedochal CystSyed Waqas HasanОценок пока нет
- Case Report 31-01-2019Документ38 страницCase Report 31-01-2019Anastanio AnugrahОценок пока нет
- Presentation Case Tuberculosis: Milda Dwi Risnandar 111170046Документ26 страницPresentation Case Tuberculosis: Milda Dwi Risnandar 111170046mildadwirisnandarОценок пока нет
- Emergency Case Reports Tuesday, February 3 2020: Surgery DepartmentДокумент22 страницыEmergency Case Reports Tuesday, February 3 2020: Surgery DepartmentAndi Nurjannah KaddirajaОценок пока нет
- Surgery Department: Emergency Case ReportsДокумент16 страницSurgery Department: Emergency Case ReportschiciОценок пока нет
- Morning Report SummaryДокумент37 страницMorning Report SummarydevyОценок пока нет
- EMCASE 6-7-2019 - EditДокумент23 страницыEMCASE 6-7-2019 - EditKomet Rama DaudОценок пока нет
- Case MalariaДокумент58 страницCase MalariaHade Guntur SОценок пока нет
- TambhanДокумент34 страницыTambhanBudiОценок пока нет
- Surgery Department: Emergency Case Reports Sunday, August 12 2018Документ36 страницSurgery Department: Emergency Case Reports Sunday, August 12 2018MukhizalОценок пока нет
- Understanding Neonatal SepsisДокумент52 страницыUnderstanding Neonatal SepsisAli FalihОценок пока нет
- Duty Report 11 Jan 2023 - RSTДокумент46 страницDuty Report 11 Jan 2023 - RSTBella AgustinОценок пока нет
- Case Report "Febrile Seizures": Betsheba E. S. 123307018Документ37 страницCase Report "Febrile Seizures": Betsheba E. S. 123307018AmandaRizkaОценок пока нет
- OB-Gyn Case Presentation - BicornuateДокумент53 страницыOB-Gyn Case Presentation - BicornuateZari Novela100% (1)
- S Kro Fulo DermaДокумент17 страницS Kro Fulo DermaAnonymous Af24L7Оценок пока нет
- Emcase 8 Juni 2019Документ38 страницEmcase 8 Juni 2019Komet Rama DaudОценок пока нет
- EMERGENCY CASE REPORTSДокумент15 страницEMERGENCY CASE REPORTSashyОценок пока нет
- Pagi Klinik Rs Usu Edit 27 Jan 2019Документ126 страницPagi Klinik Rs Usu Edit 27 Jan 2019syelsie amanda sariОценок пока нет
- PinikДокумент29 страницPinikBudiОценок пока нет
- LimfadenopatiДокумент23 страницыLimfadenopatiU TubeОценок пока нет
- Morning Report: Disusun Oleh: Devy Puspo WardoyoДокумент43 страницыMorning Report: Disusun Oleh: Devy Puspo WardoyodevyОценок пока нет
- Panik AnggitДокумент32 страницыPanik AnggitBudiОценок пока нет
- Surgery Department: Morning ReportsДокумент17 страницSurgery Department: Morning ReportsguterizalОценок пока нет
- Surgery Department: Emergency Case ReportsДокумент12 страницSurgery Department: Emergency Case ReportsMukhizalОценок пока нет
- ER Reports Detail 8 Patients TreatedДокумент12 страницER Reports Detail 8 Patients TreatedMukhizalОценок пока нет
- Gout Arthritis Case ReportДокумент55 страницGout Arthritis Case ReportikaОценок пока нет
- Case Report Typhoid Fever (A01.0)Документ32 страницыCase Report Typhoid Fever (A01.0)Alvin PratamaОценок пока нет
- OBGYN Department Duty ReportДокумент29 страницOBGYN Department Duty ReportRizkilbs LbsОценок пока нет
- Diagnosing and Treating Abdominal and Lymph Node TuberculosisДокумент22 страницыDiagnosing and Treating Abdominal and Lymph Node TuberculosisHening Tias IndianaОценок пока нет
- Morning ReportДокумент23 страницыMorning ReportBella AgustinОценок пока нет
- Laraiba SДокумент14 страницLaraiba SRizkilbs LbsОценок пока нет
- Duty Report Tuesday, January 23 2018Документ15 страницDuty Report Tuesday, January 23 2018fitra watiОценок пока нет
- Case Presentation (Brucellosis)Документ61 страницаCase Presentation (Brucellosis)Abdelrahman MokhtarОценок пока нет
- Sunday Journal - LYMДокумент23 страницыSunday Journal - LYMAlon GoldfainerОценок пока нет
- Case Presentation: Residents-In-Charge: Dr. Gonzalez/Dr. Yusingbo/Dr. Bunyi Presented By: Intern Maria Cristina S. AmatДокумент77 страницCase Presentation: Residents-In-Charge: Dr. Gonzalez/Dr. Yusingbo/Dr. Bunyi Presented By: Intern Maria Cristina S. AmatErick AncaОценок пока нет
- Chief Complaint: History TakingДокумент9 страницChief Complaint: History TakingMohamad ZulfikarОценок пока нет
- ML-acute-APДокумент20 страницML-acute-APRj PolvorosaОценок пока нет
- Progressive Muscle Wasting in a 22-Year Old FemaleДокумент25 страницProgressive Muscle Wasting in a 22-Year Old FemaleTamzid Rabby TanmoyОценок пока нет
- Bab 3 PSPДокумент108 страницBab 3 PSPSanni HuangОценок пока нет
- UTI Childhood Tadulako2015Документ38 страницUTI Childhood Tadulako2015ani bandasoОценок пока нет
- Could It Be An STI?: DR Neelam DoshiДокумент67 страницCould It Be An STI?: DR Neelam Doshijoee ahmedОценок пока нет
- PowerPoint English Case KETДокумент40 страницPowerPoint English Case KETAnonymous al0G68RwjJОценок пока нет
- Emcase 8 Juni 2019 Fix EditДокумент39 страницEmcase 8 Juni 2019 Fix EditKomet Rama DaudОценок пока нет
- Morning Report: Disusun Oleh Devy Puspo WardoyoДокумент35 страницMorning Report: Disusun Oleh Devy Puspo WardoyodevyОценок пока нет
- Fiebre Sin FocoДокумент47 страницFiebre Sin FocoTabatha Velarde ValenciaОценок пока нет
- Typhoid Fever Case ReportДокумент32 страницыTyphoid Fever Case ReportAlvin PratamaОценок пока нет
- Mekong Hernia 30 Oktober 2021Документ15 страницMekong Hernia 30 Oktober 2021Yolanda RahayuОценок пока нет
- Plasenta AkretaДокумент20 страницPlasenta AkretaHaris KurniawanОценок пока нет
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicОт EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicРейтинг: 5 из 5 звезд5/5 (1)
- Pelvic TB: Genital Tract InfectionДокумент11 страницPelvic TB: Genital Tract InfectionAmalia Zulfa AmandaОценок пока нет
- MSDS Mu-200Документ2 страницыMSDS Mu-200Goldwin Ricky Aritonang87% (15)
- Making Your Own Balms and Salves Is EasyДокумент2 страницыMaking Your Own Balms and Salves Is EasytamaraiivanaОценок пока нет
- Cough and Breathing Issues: TB, IPF, Sarcoidosis & PneumoconiosisДокумент52 страницыCough and Breathing Issues: TB, IPF, Sarcoidosis & PneumoconiosisLunaLureОценок пока нет
- APEX LithosplitДокумент30 страницAPEX Lithosplitecatalog 2018Оценок пока нет
- MCQДокумент136 страницMCQRahul Patil100% (1)
- What Does Merkaba MeanДокумент3 страницыWhat Does Merkaba MeanSubramanya SeshagiriОценок пока нет
- MidtermДокумент92 страницыMidtermPearlyn BangaanОценок пока нет
- Visual Acuity Test TEMPLATEДокумент9 страницVisual Acuity Test TEMPLATEJuriel Elohim GolvinОценок пока нет
- Clinical Treatment of Rabbits Experimentally Infected With Staphylococcus Aureus Using Different AntibioticsДокумент4 страницыClinical Treatment of Rabbits Experimentally Infected With Staphylococcus Aureus Using Different Antibioticsarum pratiwiОценок пока нет
- CoRSU Annual Report 2017Документ36 страницCoRSU Annual Report 2017Davide NaggiОценок пока нет
- HEART Grade 9Документ3 страницыHEART Grade 9Hansel MusimaОценок пока нет
- 00.040.708 - SonixTouch - Q - User - Manual PDFДокумент492 страницы00.040.708 - SonixTouch - Q - User - Manual PDFagnes septiani100% (2)
- Case StudyДокумент23 страницыCase StudyLucero HyacinthОценок пока нет
- Stock PH 28-3-2022Документ72 страницыStock PH 28-3-2022ariniОценок пока нет
- Amyloidosis: Dr. Ung Pathology Year 2Документ18 страницAmyloidosis: Dr. Ung Pathology Year 2AmniAzmiОценок пока нет
- 10 Steps Healthy Pregnancy CareДокумент5 страниц10 Steps Healthy Pregnancy CarelyiendthaОценок пока нет
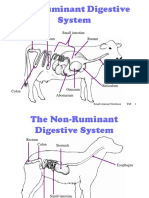
- Ruminant Digestive System ExplainedДокумент10 страницRuminant Digestive System ExplainedshivendraОценок пока нет
- 999 Giroform Perfect in Form Schunke Part1Документ12 страниц999 Giroform Perfect in Form Schunke Part1lukОценок пока нет
- Ham D PDFДокумент1 страницаHam D PDFRabiatul AdawiyahОценок пока нет
- SDS-Eng Cell Oil A Alcad June 2012Документ8 страницSDS-Eng Cell Oil A Alcad June 2012Indermohan MehtaОценок пока нет
- Philippine National Drug Policy: A Model for Science and Technology Policy-MakingДокумент10 страницPhilippine National Drug Policy: A Model for Science and Technology Policy-Makingpa3ckblancoОценок пока нет
- CARE International Brochure 13Документ40 страницCARE International Brochure 13Arun TamilvananОценок пока нет
- Febrile SeizureДокумент16 страницFebrile SeizureRashed Shatnawi100% (1)
- BioavailabilityДокумент16 страницBioavailabilityTyshanna JazzyNicole BariaОценок пока нет
- Gastroenterology: Maintenance of Certification (MOC) Examination BlueprintДокумент11 страницGastroenterology: Maintenance of Certification (MOC) Examination BlueprintAdson AlcantaraОценок пока нет
- ADA Caries Risk Assessment Form Completion Instructions PDFДокумент3 страницыADA Caries Risk Assessment Form Completion Instructions PDFDavid ColonОценок пока нет
- Completed Hse+3704+curriculum+development+workbook++section+a +introductionДокумент14 страницCompleted Hse+3704+curriculum+development+workbook++section+a +introductionapi-2814357340% (1)
- Step by Step Construction of Orthodontic Removable ApplianceДокумент49 страницStep by Step Construction of Orthodontic Removable Applianceآلاء حسن يونسОценок пока нет
- Formulation and Evaluation of Wood Apple Supplemented KalakandДокумент3 страницыFormulation and Evaluation of Wood Apple Supplemented KalakandDr-Prafull Pratap Singh YadavОценок пока нет