Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Sweet Emotion: Bass Line ForДокумент2 страницыSweet Emotion: Bass Line ForJames Gale100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Reading Comprehension Animals Copyright English Created Resources PDFДокумент10 страницReading Comprehension Animals Copyright English Created Resources PDFCasillas ElОценок пока нет
- Phonetics Exercises PDFДокумент2 страницыPhonetics Exercises PDFShanti YuliastitiОценок пока нет
- UCO Reporter 2021, December Edition, November 26, 2021Документ40 страницUCO Reporter 2021, December Edition, November 26, 2021ucopresident100% (2)
- Safety Guidelines For Direct DrivesДокумент9 страницSafety Guidelines For Direct DrivesJOseОценок пока нет
- 2 Fluid and Electrolyte AbnormalityДокумент16 страниц2 Fluid and Electrolyte AbnormalityGoez Aditya NugrahaОценок пока нет
- CES Wrong Answer SummaryДокумент4 страницыCES Wrong Answer SummaryZorg UAОценок пока нет
- Global High Temperature Grease Market ReportДокумент6 страницGlobal High Temperature Grease Market ReportHari PurwadiОценок пока нет
- (PDF) Download Modern Architecture Since 1900 PDF Ebook by William J.RДокумент2 страницы(PDF) Download Modern Architecture Since 1900 PDF Ebook by William J.Rkhushboov98296% (16)
- (AC-S08) Week 08 - Pre-Task - Quiz - Weekly Quiz - INGLES III (14653)Документ3 страницы(AC-S08) Week 08 - Pre-Task - Quiz - Weekly Quiz - INGLES III (14653)Eduardo Arucutipa60% (5)
- 8.new Daftar Pustaka Tesis IbanДокумент4 страницы8.new Daftar Pustaka Tesis IbanGoez Aditya NugrahaОценок пока нет
- Triglyceride Ratio and Cardiovascular Risk in DiabetesДокумент9 страницTriglyceride Ratio and Cardiovascular Risk in DiabetesGoez Aditya NugrahaОценок пока нет
- Revisi Slide Adb Lecture Koass - Dwi AДокумент23 страницыRevisi Slide Adb Lecture Koass - Dwi AGoez Aditya NugrahaОценок пока нет
- ECG Interpretation GuideДокумент44 страницыECG Interpretation GuideGoez Aditya NugrahaОценок пока нет
- All Cydex Squad Plus NimДокумент7 страницAll Cydex Squad Plus NimGoez Aditya NugrahaОценок пока нет
- Tentative On Going 2017-03-22 Jam 16.30Документ3 страницыTentative On Going 2017-03-22 Jam 16.30Goez Aditya NugrahaОценок пока нет
- DASAR-DASAR DIAGNOSIS HEPATITIS B KRONIS - 106. (Dasar-Dasar Diagnosis Hepatitis B Kronis)Документ50 страницDASAR-DASAR DIAGNOSIS HEPATITIS B KRONIS - 106. (Dasar-Dasar Diagnosis Hepatitis B Kronis)ayudilaОценок пока нет
- Draft Acc Text Book Nefro DR Wayan SudhanaДокумент1 страницаDraft Acc Text Book Nefro DR Wayan SudhanaGoez Aditya NugrahaОценок пока нет
- IV Drug Drip Calculation FormulasДокумент10 страницIV Drug Drip Calculation FormulasGoez Aditya NugrahaОценок пока нет
- Pendidikan Kedokteran Berkelanjutan (PKB) XXV - Trigonum Sudema Ilmu Penyakit Dalam FK Unud/Rsup Sanglah 2017Документ5 страницPendidikan Kedokteran Berkelanjutan (PKB) XXV - Trigonum Sudema Ilmu Penyakit Dalam FK Unud/Rsup Sanglah 2017Goez Aditya NugrahaОценок пока нет
- HIV Multi-Drug ResistanceДокумент10 страницHIV Multi-Drug ResistanceGoez Aditya NugrahaОценок пока нет
- 4 Corticosteroid Dose EquivalentДокумент2 страницы4 Corticosteroid Dose EquivalentGoez Aditya NugrahaОценок пока нет
- Correlation of Visceral Fat Level Towards Poor Cognitive Function Among Elderly Patient in DenpasarДокумент12 страницCorrelation of Visceral Fat Level Towards Poor Cognitive Function Among Elderly Patient in DenpasarGoez Aditya NugrahaОценок пока нет
- Guia TromboprofilaxisДокумент41 страницаGuia TromboprofilaxisAnaili NimzaОценок пока нет
- Opt-Sanglah POLI KoepietДокумент18 страницOpt-Sanglah POLI KoepietGoez Aditya NugrahaОценок пока нет
- AnastesiДокумент1 страницаAnastesiGoez Aditya NugrahaОценок пока нет
- Judul SS3 Cydex AllДокумент125 страницJudul SS3 Cydex AllGoez Aditya Nugraha100% (1)
- Tribal Ethics of Mizo and Ao NagasДокумент8 страницTribal Ethics of Mizo and Ao NagasVincent TharteaОценок пока нет
- Kimone Wright - Registered Nurse ResumeДокумент2 страницыKimone Wright - Registered Nurse Resumeapi-365123958Оценок пока нет
- Miles and Snow's Organizational StrategiesДокумент15 страницMiles and Snow's Organizational StrategiesVirat SahОценок пока нет
- Diagnostic Test in Mapeh 8: Department of EducationДокумент4 страницыDiagnostic Test in Mapeh 8: Department of Educationcarl jayОценок пока нет
- One Stop Report - Tata MotorsДокумент119 страницOne Stop Report - Tata MotorsJia HuiОценок пока нет
- A Project Report On Working Capital Management of Hindalco For The Last Five YearsДокумент83 страницыA Project Report On Working Capital Management of Hindalco For The Last Five YearsBabasab Patil (Karrisatte)0% (1)
- Revised Organizational Structure of Railway BoardДокумент4 страницыRevised Organizational Structure of Railway BoardThirunavukkarasu ThirunavukkarasuОценок пока нет
- Alan Ross CV Expert Road Safety AdviserДокумент4 страницыAlan Ross CV Expert Road Safety AdviserAnna Sophia YorkОценок пока нет
- MATHS UNDERSTANDINGДокумент15 страницMATHS UNDERSTANDINGNurul IzzaОценок пока нет
- Pines City Colleges: College of NursingДокумент2 страницыPines City Colleges: College of NursingmagisasamundoОценок пока нет
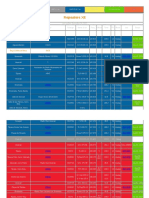
- Repeaters XE PDFДокумент12 страницRepeaters XE PDFenzzo molinariОценок пока нет
- Igbo Traditional Security System: A Panacea To Nigeria Security QuagmireДокумент17 страницIgbo Traditional Security System: A Panacea To Nigeria Security QuagmireChukwukadibia E. Nwafor100% (1)
- Station 6 Part 1 2Документ4 страницыStation 6 Part 1 2api-292196043Оценок пока нет
- Talha Farooqi - Assignment 01 - Overview of Bond Sectors and Instruments - Fixed Income Analysis PDFДокумент4 страницыTalha Farooqi - Assignment 01 - Overview of Bond Sectors and Instruments - Fixed Income Analysis PDFMohammad TalhaОценок пока нет
- Noise Pollution Control Policy IndiaДокумент10 страницNoise Pollution Control Policy IndiaAllu GiriОценок пока нет
- Rational design of Nile bargesДокумент8 страницRational design of Nile bargesjhairОценок пока нет
- Nursing ManagementДокумент14 страницNursing ManagementNolan Ivan EudinОценок пока нет
- Contoh Format Soal PTSДокумент3 страницыContoh Format Soal PTSSmp nasional plus widiatmikaОценок пока нет
- Jeff Roth CVДокумент3 страницыJeff Roth CVJoseph MooreОценок пока нет
- Unit 3 Administrative AdjudicationДокумент18 страницUnit 3 Administrative AdjudicationkipkarОценок пока нет
- Slope StabilityДокумент11 страницSlope StabilityAhmed MohebОценок пока нет