Вам также может понравиться
- Parotid 121206120631 Phpapp01Документ26 страницParotid 121206120631 Phpapp01shravani100% (1)
- Superficial ParotidectomyДокумент7 страницSuperficial ParotidectomySajid Hussain ShahОценок пока нет
- Neck Dissection: Jeffrey Buyten, MD Susan Mccammon, MD Francis B. Quinn, MDДокумент60 страницNeck Dissection: Jeffrey Buyten, MD Susan Mccammon, MD Francis B. Quinn, MDentgo8282Оценок пока нет
- Parotidectomy: H.Shameer AhamedДокумент47 страницParotidectomy: H.Shameer AhamedAndreas RendraОценок пока нет
- ParotidectomyДокумент10 страницParotidectomyFahad QiamОценок пока нет
- Neck Dissection 020116 Slides PDFДокумент139 страницNeck Dissection 020116 Slides PDFHeru IskandarОценок пока нет
- Breast Reconstruction After Mastectomy For Breast Tumor: About 24 CasesДокумент6 страницBreast Reconstruction After Mastectomy For Breast Tumor: About 24 CasesIJAR JOURNALОценок пока нет
- Oral LymphangiomaДокумент8 страницOral LymphangiomasevattapillaiОценок пока нет
- Neoplastic Thyroid Disease - Thyroid Nodules Goiter and Thyroid CancerДокумент57 страницNeoplastic Thyroid Disease - Thyroid Nodules Goiter and Thyroid CancerNavya SreeОценок пока нет
- Local and Regional Flaps-1Документ89 страницLocal and Regional Flaps-1Bilal Basit100% (1)
- Vascular Anomalies PresentationДокумент45 страницVascular Anomalies PresentationMhinory OctОценок пока нет
- Excision of Preauricular Pits and SinusesДокумент7 страницExcision of Preauricular Pits and SinusesHОценок пока нет
- Anorectal Surgery PDFДокумент33 страницыAnorectal Surgery PDFLuminitaDumitriuОценок пока нет
- Cervicofacial LymphangiomasДокумент11 страницCervicofacial LymphangiomasCharmila Sari100% (1)
- Open Access Atlas of Otolaryngology, Head & Neck Operative SurgeryДокумент12 страницOpen Access Atlas of Otolaryngology, Head & Neck Operative Surgerysavyasachin100% (1)
- Petrous ApexДокумент6 страницPetrous ApexSarat Kumar ChalasaniОценок пока нет
- Ranula - A Case ReportДокумент2 страницыRanula - A Case Reportnnmey20100% (1)
- Nasolabial Flap For Oral Cavity ReconstructionДокумент10 страницNasolabial Flap For Oral Cavity ReconstructionJamesОценок пока нет
- Edh, SDH, & Burr HolesДокумент46 страницEdh, SDH, & Burr HolesRully Riyan DikaОценок пока нет
- Submandibular Gland ExcisionДокумент8 страницSubmandibular Gland ExcisiondrdilberОценок пока нет
- Benign Tumours of LarynxДокумент35 страницBenign Tumours of LarynxMidhun Thomas EdathinalОценок пока нет
- Surgical Anatomy Related To Skull Base SurgeryДокумент24 страницыSurgical Anatomy Related To Skull Base Surgeryeldoc13Оценок пока нет
- Augmentation Mammoplasty:MastopexyДокумент12 страницAugmentation Mammoplasty:MastopexyfumblefumbleОценок пока нет
- Mylo Anal StenosisДокумент8 страницMylo Anal StenosisCarmen DiazОценок пока нет
- Anatomy of The Parapharyngeal SpaceДокумент10 страницAnatomy of The Parapharyngeal SpaceNariska CooperОценок пока нет
- Radical Neck Dissection: (RND) Classification, Indication and TechniquesДокумент42 страницыRadical Neck Dissection: (RND) Classification, Indication and TechniquesPatrycyaОценок пока нет
- Primary Haemangioma of The Skull: Case ReviewДокумент3 страницыPrimary Haemangioma of The Skull: Case ReviewSoemantri Doank100% (1)
- Surgical Anatomy of Facial NerveДокумент34 страницыSurgical Anatomy of Facial NerveKunal ChandnaniОценок пока нет
- Tumours of HypopharynxДокумент32 страницыTumours of HypopharynxDurrikamil khattakОценок пока нет
- Radial Forearm Flap: DR G Avinash Rao Fellow Hand and Microsurgery Skims, SrinagarДокумент71 страницаRadial Forearm Flap: DR G Avinash Rao Fellow Hand and Microsurgery Skims, Srinagaravinashrao39Оценок пока нет
- Salivary Gland TumorДокумент62 страницыSalivary Gland Tumordeepak kumarОценок пока нет
- 24 Olsen Variations ParotidectomyДокумент33 страницы24 Olsen Variations ParotidectomyAngga Witra NandaОценок пока нет
- Surgical Resection of Cancer of The Buccal MucosaДокумент21 страницаSurgical Resection of Cancer of The Buccal MucosapradeepОценок пока нет
- Parotid Tumors and Other Salivary Gland TumorsДокумент41 страницаParotid Tumors and Other Salivary Gland Tumorsdrhiwaomer100% (9)
- Cyst Neck Tumor (DR Bob Andinata)Документ33 страницыCyst Neck Tumor (DR Bob Andinata)Intan Eklesiana NapitupuluОценок пока нет
- Sphenopalatine Artery - SPA - LigationДокумент5 страницSphenopalatine Artery - SPA - LigationHossam Elden Helmy HaridyОценок пока нет
- Surgical Management of Thyroid NeoplasmsДокумент15 страницSurgical Management of Thyroid NeoplasmsalameluОценок пока нет
- Facial NerveДокумент45 страницFacial NerveyudhafpОценок пока нет
- Lymphatic Drainage of Breast FINALДокумент30 страницLymphatic Drainage of Breast FINALMuhammad Azhar Qureshi100% (1)
- Anal ProblemsДокумент35 страницAnal ProblemsSandip VaghelaОценок пока нет
- Neckdissections 130421031843 Phpapp02Документ62 страницыNeckdissections 130421031843 Phpapp02azizОценок пока нет
- Erb's PointДокумент14 страницErb's PointRohit SharmaОценок пока нет
- Parotid TumorДокумент37 страницParotid TumorRiyan SaputraОценок пока нет
- 14 Anterolateral Thigh FlapДокумент6 страниц14 Anterolateral Thigh FlapAngga Putra100% (1)
- Superficial Parotidectomy Through Retrograde Facial Nerve DissectionДокумент8 страницSuperficial Parotidectomy Through Retrograde Facial Nerve DissectionAnonymous LnWIBo1GОценок пока нет
- Deltopectoral FlapДокумент37 страницDeltopectoral FlapAmbika Luthra100% (1)
- 2010 Facial Degloving Approach To The MidfaceДокумент4 страницы2010 Facial Degloving Approach To The MidfaceAFJimenezOОценок пока нет
- BeraДокумент20 страницBeraMuhamad SyaifulОценок пока нет
- Skinflaps: Mary Tschoi,, Erik A. Hoy,, Mark S. GranickДокумент16 страницSkinflaps: Mary Tschoi,, Erik A. Hoy,, Mark S. Granickdanico59Оценок пока нет
- Open SeptorhinoplastyДокумент6 страницOpen SeptorhinoplastybarbiemeОценок пока нет
- Precancerous Conditions of Oral CavityДокумент80 страницPrecancerous Conditions of Oral Cavitylarisabrinza12Оценок пока нет
- Local and Regional Flaps in Head and Neck Cancer / Orthodontic Courses by Indian Dental AcademyДокумент56 страницLocal and Regional Flaps in Head and Neck Cancer / Orthodontic Courses by Indian Dental Academyindian dental academyОценок пока нет
- Thyroidectomy Vula AtlasДокумент15 страницThyroidectomy Vula AtlasyvonneОценок пока нет
- NeckdissectionsДокумент130 страницNeckdissectionsAlvaro RivCalleОценок пока нет
- Soft Tissue SarcomaДокумент45 страницSoft Tissue SarcomaWadhe TobingОценок пока нет
- Rhinoplasty WorkbookДокумент21 страницаRhinoplasty Workbookzena talibОценок пока нет
- A System of Operative Surgery, Volume IV (of 4)От EverandA System of Operative Surgery, Volume IV (of 4)Рейтинг: 4 из 5 звезд4/5 (1)
- ParotidectomyДокумент28 страницParotidectomyGede HendraОценок пока нет
- TRIGONUM RevisiДокумент5 страницTRIGONUM RevisidokteraanОценок пока нет
- 12 DHF DRДокумент56 страниц12 DHF DRdokteraanОценок пока нет
- Pemeriksaan Fisik Kepala Dan LeherДокумент39 страницPemeriksaan Fisik Kepala Dan LeherdokteraanОценок пока нет
- Pelvic Fracture-Related Injuries of The Bladder Neck andДокумент12 страницPelvic Fracture-Related Injuries of The Bladder Neck anddokteraanОценок пока нет
- Hotchkiss 2013Документ13 страницHotchkiss 2013dokteraanОценок пока нет
- Abdominal Anatomy For GIST: The Peritoneum and RetroperitoneumДокумент5 страницAbdominal Anatomy For GIST: The Peritoneum and RetroperitoneumdokteraanОценок пока нет
- Output PathДокумент4 страницыOutput PathdokteraanОценок пока нет
- Compartment SyndromeДокумент14 страницCompartment SyndromedokteraanОценок пока нет
- Decompressive Craniectomy (For Severe Head Injury) : A Patient / Family Informed Consent Guide ToДокумент8 страницDecompressive Craniectomy (For Severe Head Injury) : A Patient / Family Informed Consent Guide TodokteraanОценок пока нет
- Cancer Is An Abnormal Disorganised Growth of Cells in The: PrintДокумент1 страницаCancer Is An Abnormal Disorganised Growth of Cells in The: Printshailesh284Оценок пока нет
- Acute Limb Ischemia SiteДокумент23 страницыAcute Limb Ischemia Sitedokteraan100% (2)
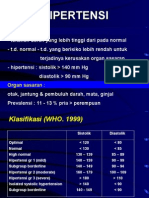
- HipertensiДокумент28 страницHipertensidokteraanОценок пока нет
- CUPS Pediatric Trauma EvaluationДокумент2 страницыCUPS Pediatric Trauma EvaluationdokteraanОценок пока нет
- Good Surgical PracticeДокумент10 страницGood Surgical PracticedokteraanОценок пока нет
- Reference LetterДокумент2 страницыReference LetterdokteraanОценок пока нет
- TAFE SA Application Document Cover Sheet Attach A Copy of This Cover Sheet To Any Documents You Submit To SATACДокумент1 страницаTAFE SA Application Document Cover Sheet Attach A Copy of This Cover Sheet To Any Documents You Submit To SATACdokteraanОценок пока нет
- M Communication 111Документ14 страницM Communication 111dokteraanОценок пока нет
- Pace MakerДокумент24 страницыPace Makerدرة عبداللهОценок пока нет
- (Neuromethods 150) Marco Cascella - General Anesthesia Research-Springer US - Humana (2020) PDFДокумент259 страниц(Neuromethods 150) Marco Cascella - General Anesthesia Research-Springer US - Humana (2020) PDFCristian C BecerraОценок пока нет
- Deformities: Karl V. Bustamante Johara Micah RegidorДокумент28 страницDeformities: Karl V. Bustamante Johara Micah Regidorcharlo_camachoОценок пока нет
- Applications of Gait Analysis in Pediatric Orthopaedics: Current Orthopaedic Practice May 2016Документ11 страницApplications of Gait Analysis in Pediatric Orthopaedics: Current Orthopaedic Practice May 2016Selina Kayelin Go-LimОценок пока нет
- Evaluation of Nurses Knowledge Levels of DiabeticДокумент13 страницEvaluation of Nurses Knowledge Levels of DiabeticKlinik KitamuraОценок пока нет
- MalariaДокумент22 страницыMalariaAbdirahmanОценок пока нет
- Rep MainДокумент2 страницыRep MainKaran SinghОценок пока нет
- Heart Failure COncept MapДокумент2 страницыHeart Failure COncept MapJrBong SemaneroОценок пока нет
- Models of PreventionДокумент13 страницModels of Preventionsagi mu100% (1)
- Thesis Dental Public HealthДокумент8 страницThesis Dental Public Healthbsem160v100% (2)
- Dietary Computations PPT LabДокумент22 страницыDietary Computations PPT LabCathy Dao-ayenОценок пока нет
- Penyakit Berjangkit Di Kalangan Penagih Heroin Yang Menerima Rawatan Pesakit Luar Di MuarДокумент8 страницPenyakit Berjangkit Di Kalangan Penagih Heroin Yang Menerima Rawatan Pesakit Luar Di MuarPenjejak BadaiОценок пока нет
- Dog Acupressure Chart and Pressure PointsДокумент6 страницDog Acupressure Chart and Pressure PointsLaura As GpОценок пока нет
- Mental Health, Physical Activity and Physical Therapy: ExerciseДокумент8 страницMental Health, Physical Activity and Physical Therapy: ExerciseMoVaEm7Оценок пока нет
- Scleroderma, Sjogren's SyndromeДокумент31 страницаScleroderma, Sjogren's SyndromeSalomeSibashviliОценок пока нет
- Support GroupsДокумент5 страницSupport Groupsapi-364431775Оценок пока нет
- IGNOU Block 3 Unit 4 Communicable Diseases 3 - Zoonotic DiseasesДокумент17 страницIGNOU Block 3 Unit 4 Communicable Diseases 3 - Zoonotic Diseaseserice.researchОценок пока нет
- Cholesterol CPДокумент6 страницCholesterol CPLAB. GATOT SUBROTOОценок пока нет
- Clinical Education: Interpretation of AbgsДокумент8 страницClinical Education: Interpretation of AbgsRumela Ganguly ChakrabortyОценок пока нет
- FORENSIC 5 WEEK 4 Students Copy 2023Документ68 страницFORENSIC 5 WEEK 4 Students Copy 2023Grczhl GornesОценок пока нет
- Advance Nutrition CourseДокумент2 страницыAdvance Nutrition CoursedigitalfunОценок пока нет
- Target200plus Test Series December 2023Документ8 страницTarget200plus Test Series December 2023Lijo JoОценок пока нет
- Unit 05 (A) Cardiac Glycosides, Educational PlatformДокумент41 страницаUnit 05 (A) Cardiac Glycosides, Educational PlatformSajid AhmadОценок пока нет
- Global Statistics Avian InfluenzaДокумент2 страницыGlobal Statistics Avian InfluenzaSatria KinoОценок пока нет
- SpedДокумент19 страницSpedLyra CampbilОценок пока нет
- Transcript Foundational Herbcraft Part 1Документ32 страницыTranscript Foundational Herbcraft Part 1Stacey DianeОценок пока нет
- Coronavirus Survival - Final by Ted PollardДокумент37 страницCoronavirus Survival - Final by Ted PollardthereadingshelfОценок пока нет
- From Bite To Mind: TMD - A Personal and Literature Review: Carl Molin, LDS, Odont DTДокумент11 страницFrom Bite To Mind: TMD - A Personal and Literature Review: Carl Molin, LDS, Odont DTDrDejanDrakulОценок пока нет
- Kazdin, 2015Документ8 страницKazdin, 2015Elizabeth Roxan Lizaso GonzálezОценок пока нет
- Disease ControlДокумент20 страницDisease Controlbibi bennyОценок пока нет