Вам также может понравиться
- Management of DiarrhoeaДокумент16 страницManagement of Diarrhoeasunday danielОценок пока нет
- 2.6.3.7 Irritable Bowel Syndrom &kolitisДокумент48 страниц2.6.3.7 Irritable Bowel Syndrom &kolitisVaniОценок пока нет
- 1 sec GERD GITДокумент85 страниц1 sec GERD GITtyleree3Оценок пока нет
- Disorders of the Stomach and Intestines GuideДокумент64 страницыDisorders of the Stomach and Intestines GuideAyomide IgeОценок пока нет
- Malnutrisi GeriatriДокумент35 страницMalnutrisi GeriatriselymariaОценок пока нет
- GastrointestinaldrugsДокумент30 страницGastrointestinaldrugsmayaОценок пока нет
- IBS: A Guide to Irritable Bowel SyndromeДокумент38 страницIBS: A Guide to Irritable Bowel SyndromeMuhammed sherbinОценок пока нет
- Lec 2 - GIT DrugsДокумент68 страницLec 2 - GIT DrugsAiqa QaziОценок пока нет
- 5a.ESOPHAGEAL DISORDERSДокумент16 страниц5a.ESOPHAGEAL DISORDERSHayat AL AKOUMОценок пока нет
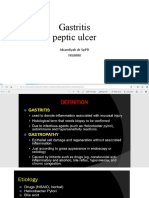
- Session 20-Gastritis and PudДокумент42 страницыSession 20-Gastritis and Pudgbunyara100Оценок пока нет
- Acid Peptic Disorder and GerdДокумент52 страницыAcid Peptic Disorder and GerdEbuka AniОценок пока нет
- GERD ManagementДокумент43 страницыGERD ManagementpashaОценок пока нет
- Dr. Mamun's Guide to Evaluating DyspepsiaДокумент35 страницDr. Mamun's Guide to Evaluating DyspepsiaZahraa MurtadaОценок пока нет
- Drug Induced DiarrhoeaДокумент18 страницDrug Induced DiarrhoeaNikhil Gupta0% (1)
- hs320 W11 DigestiveSystemDisordersДокумент41 страницаhs320 W11 DigestiveSystemDisordersjoseyalm2323Оценок пока нет
- Irritable Bowel Syndrome 2Документ61 страницаIrritable Bowel Syndrome 2MoonОценок пока нет
- Medications in Inflammatory Bowel Diseases pptДокумент49 страницMedications in Inflammatory Bowel Diseases pptgitama9904Оценок пока нет
- Drug StudyДокумент6 страницDrug StudyMiru มิริวОценок пока нет
- GERDДокумент38 страницGERDss33% (3)
- GIT Disordeer DentistДокумент107 страницGIT Disordeer DentistNasser SalahОценок пока нет
- Farmakoterapi Gastroenteritis: Widyati Farmasis Klinik Rsal DR RamelanДокумент17 страницFarmakoterapi Gastroenteritis: Widyati Farmasis Klinik Rsal DR RamelanViona PrasetyoОценок пока нет
- Drug OrderДокумент8 страницDrug OrderRiezza BalicaoОценок пока нет
- Stomach &duodenumДокумент89 страницStomach &duodenumj6r4qvkrkzОценок пока нет
- Medications Used in diarrhoea pptДокумент25 страницMedications Used in diarrhoea pptgitama9904Оценок пока нет
- Pharmacotherapy of GERDДокумент33 страницыPharmacotherapy of GERDFahril LabuduОценок пока нет
- Gastroesophageal RefluxДокумент20 страницGastroesophageal Refluxtofan widyaОценок пока нет
- AzithromycinДокумент3 страницыAzithromycinapi-3797941100% (2)
- Pharmacotherapy 1 GIS Self CarepdfДокумент40 страницPharmacotherapy 1 GIS Self Carepdfelifuygur09Оценок пока нет
- Dyspepsia and Gastritis GuideДокумент80 страницDyspepsia and Gastritis GuideSoumya Ranjan PandaОценок пока нет
- BioДокумент18 страницBioKinza ZubairОценок пока нет
- PudДокумент20 страницPudSINDHOOR S MОценок пока нет
- Pharmacology of GIT: Drugs Used in Peptic Ulcer TreatmentДокумент29 страницPharmacology of GIT: Drugs Used in Peptic Ulcer TreatmentMohammed Bahnasy100% (1)
- T HypoidДокумент22 страницыT HypoidDeddy ShangrelaОценок пока нет
- Ward6 Drug StudyДокумент6 страницWard6 Drug StudyMichael Lloyd T. SabijonОценок пока нет
- Unit 3 Gastrointestinal SystemДокумент12 страницUnit 3 Gastrointestinal SystemdhanashriОценок пока нет
- 5.5 GI Disorders Dr. Jison 2022Документ72 страницы5.5 GI Disorders Dr. Jison 2022Monique BorresОценок пока нет
- DR/ Mohammad Abdul Baset Badr: Prepared byДокумент75 страницDR/ Mohammad Abdul Baset Badr: Prepared byamrharidi446Оценок пока нет
- GASTRITISДокумент16 страницGASTRITISLokeshwari KatreОценок пока нет
- Evaluation of GIT Dr. Bereket Molla TigabuДокумент44 страницыEvaluation of GIT Dr. Bereket Molla Tigabuphoto copyhemnОценок пока нет
- DOC-20240110-WA0016.Документ176 страницDOC-20240110-WA0016.Sreeja ReddyОценок пока нет
- Gastrointestinal Medicines MBCHB II - 2023 NdlovuДокумент31 страницаGastrointestinal Medicines MBCHB II - 2023 NdlovuKeamogetswe Zwane100% (1)
- Disorders of The Gastrointestinal System: Dody Taruna, DR, MkesДокумент62 страницыDisorders of The Gastrointestinal System: Dody Taruna, DR, Mkeserick djuandaОценок пока нет
- StomachДокумент86 страницStomachSuneel Kaushik KОценок пока нет
- Nichols GI 09Документ59 страницNichols GI 09marviecute22Оценок пока нет
- GI DrugsДокумент35 страницGI DrugsIconMaicoОценок пока нет
- Gastritis and Peptic Ulcer 1Документ26 страницGastritis and Peptic Ulcer 1AqshaОценок пока нет
- Lecture 1part 2Документ50 страницLecture 1part 2mashe1Оценок пока нет
- Management Peptic UlcerДокумент11 страницManagement Peptic Ulcertofan widyaОценок пока нет
- Geriatric Giants Iwal 1 2020Документ58 страницGeriatric Giants Iwal 1 2020selymariaОценок пока нет
- GERD.pptxДокумент20 страницGERD.pptxSINDHOOR S MОценок пока нет
- Drugs For Diarrhea and ConstipationДокумент24 страницыDrugs For Diarrhea and ConstipationFaddi BoyОценок пока нет
- Drugs Affecting The Gastrointestinal TractДокумент61 страницаDrugs Affecting The Gastrointestinal TractSameera DahamОценок пока нет
- Lecture 21 Drugs Against GI DisordersДокумент40 страницLecture 21 Drugs Against GI DisordershamzabhayatОценок пока нет
- Gangguan GastrointestinalДокумент62 страницыGangguan GastrointestinalHello SunshineОценок пока нет
- By: Clarissa E. Guifaya BSN301/GROUP 3Документ17 страницBy: Clarissa E. Guifaya BSN301/GROUP 3Clarissa GuifayaОценок пока нет
- Acute and Chronic GastritisДокумент17 страницAcute and Chronic GastritisIndah Nur PratiwiОценок пока нет
- A Simple Guide to Gastritis and Related ConditionsОт EverandA Simple Guide to Gastritis and Related ConditionsРейтинг: 4.5 из 5 звезд4.5/5 (3)
- The Ultimate Gastroparesis Diet Cookbook:The Complete Nutrition Guide To Help Treat And Manage Gastroparesis With Delectable And Nourishing RecipesОт EverandThe Ultimate Gastroparesis Diet Cookbook:The Complete Nutrition Guide To Help Treat And Manage Gastroparesis With Delectable And Nourishing RecipesОценок пока нет
- Gastrointestinal Health: The Self-Help Nutritional Program That Can Change the Lives of 80 Million AmericansОт EverandGastrointestinal Health: The Self-Help Nutritional Program That Can Change the Lives of 80 Million AmericansОценок пока нет
- YOKOGAWAДокумент16 страницYOKOGAWADavide ContiОценок пока нет
- 2.gantry Rotation Safety CheckДокумент2 страницы2.gantry Rotation Safety CheckLê Hồ Nguyên ĐăngОценок пока нет
- Ethics Module 2 - NotesДокумент1 страницаEthics Module 2 - Notesanon_137579236Оценок пока нет
- Porta by AmbarrukmoДокумент4 страницыPorta by AmbarrukmoRika AyuОценок пока нет
- Vishwabhanu Oct '18 - Jan '19Документ26 страницVishwabhanu Oct '18 - Jan '19vedicvision99100% (3)
- SmartRunway SmartLandingДокумент39 страницSmartRunway SmartLandingMikeОценок пока нет
- Three Bucket Method & Food ServiceДокумент4 страницыThree Bucket Method & Food Servicerose zandrea demasisОценок пока нет
- IIT2019 RIT-1-CPM Chemistry TestДокумент15 страницIIT2019 RIT-1-CPM Chemistry TestPRAKHAR GUPTAОценок пока нет
- MUCLecture 2021 10311889Документ11 страницMUCLecture 2021 10311889Ramon Angelo MendezОценок пока нет
- Takara 2012Документ57 страницTakara 2012Deepak Ranjan SahooОценок пока нет
- Overlord - Volume 01 - The Undead KingДокумент223 страницыOverlord - Volume 01 - The Undead KingPaulo FordheinzОценок пока нет
- GSM Modernization Poster2Документ1 страницаGSM Modernization Poster2leonardomarinОценок пока нет
- BS en 12201 5 2011Документ20 страницBS en 12201 5 2011fatjon31100% (4)
- Supply Chain Management: Tata Tea's Global OperationsДокумент15 страницSupply Chain Management: Tata Tea's Global OperationsAmit Halder 2020-22Оценок пока нет
- Director's Report Highlights Record Wheat Production in IndiaДокумент80 страницDirector's Report Highlights Record Wheat Production in Indiakamlesh tiwariОценок пока нет
- Cooling System Exhaust System: RadiatorДокумент2 страницыCooling System Exhaust System: RadiatorMd ShОценок пока нет
- IMRAD - G1 PepperДокумент13 страницIMRAD - G1 PepperRomero, Ken Angelo B.Оценок пока нет
- Causes and Effects of PollutionДокумент6 страницCauses and Effects of PollutionNhư NgọcОценок пока нет
- Edexcel A-Level Biology Experimental Design Marks Scheme (1) (Full Permission)Документ16 страницEdexcel A-Level Biology Experimental Design Marks Scheme (1) (Full Permission)FardeenKhanОценок пока нет
- Orientation Report PDFДокумент13 страницOrientation Report PDFRiaz RasoolОценок пока нет
- Print Date:: Container No NO Size Seal No Seal Party Supplier Status Movement TypeДокумент3 страницыPrint Date:: Container No NO Size Seal No Seal Party Supplier Status Movement TypeYudha PermanaОценок пока нет
- EiaДокумент14 страницEiaRamir FamorcanОценок пока нет
- 6b530300 04f6 40b9 989e Fd39aaa6293aДокумент1 страница6b530300 04f6 40b9 989e Fd39aaa6293attariq_jjavedОценок пока нет
- ME 2141 - Complete ModuleДокумент114 страницME 2141 - Complete ModuleNICOLE ANN MARCELINOОценок пока нет
- Advanced Composite Materials Design EngineeringДокумент19 страницAdvanced Composite Materials Design EngineeringpanyamnrОценок пока нет
- LIST Real Estate Contacts ListДокумент4 страницыLIST Real Estate Contacts ListChauhan Harshit100% (1)
- Finals-Insurance Week 5Документ19 страницFinals-Insurance Week 5Ryan ChristianОценок пока нет
- Lab Manual Cape Bio Unit 1 2023Документ37 страницLab Manual Cape Bio Unit 1 2023drug123addict25Оценок пока нет
- 18 Butterfly Valves A Disc BrayДокумент10 страниц18 Butterfly Valves A Disc BrayAli FananiОценок пока нет
- Citric Acid Passivation of Stainless SteelДокумент41 страницаCitric Acid Passivation of Stainless Steelnqh2009100% (2)